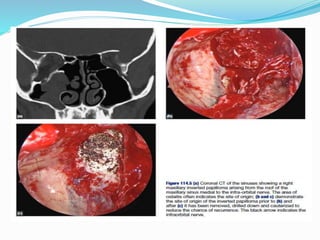
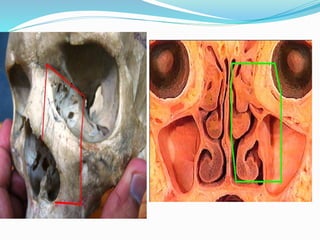
1. Inverted papilloma is a benign epithelial tumor originating from the Schneiderian membrane of the nasal cavity and paranasal sinuses.
2. It most commonly affects males ages 30-50 and presents as a unilateral nasal mass, obstruction, and bleeding.
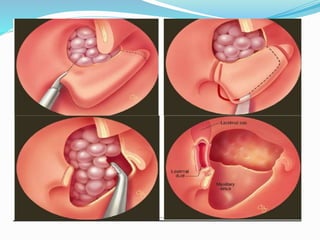
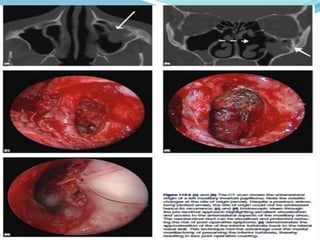
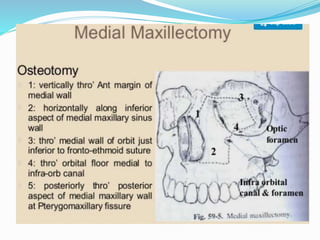
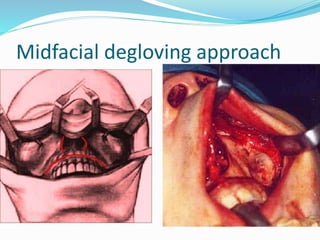
3. Treatment involves surgical resection, typically an endoscopic medial maxillectomy to remove the entire lateral nasal wall and clear the tumor attachment site.
























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



