Downloaded 55 times


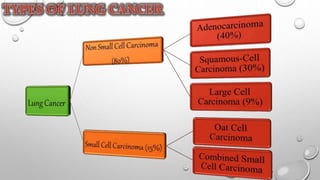
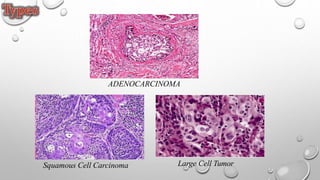
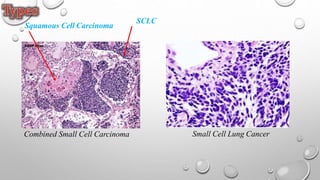
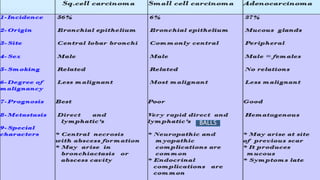
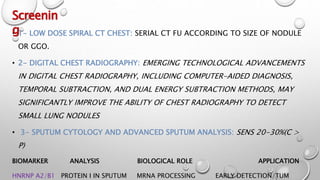
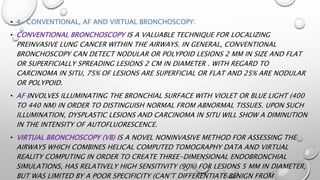
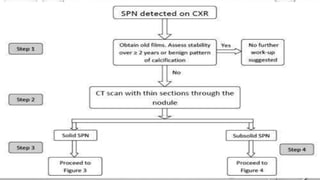
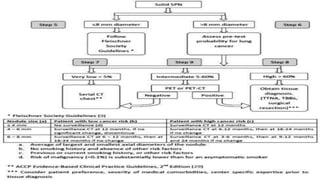
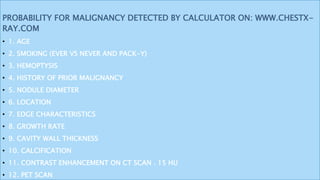
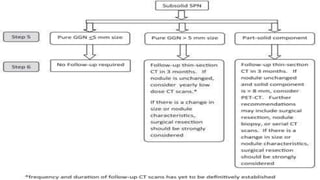
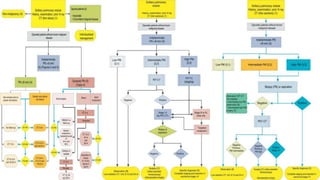
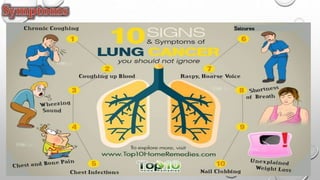
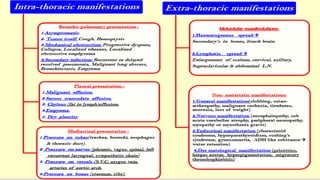
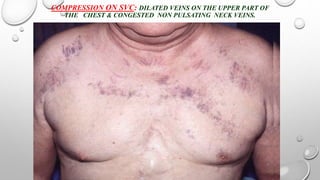
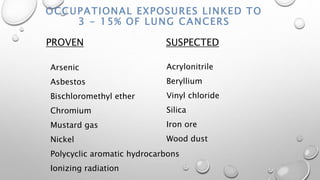
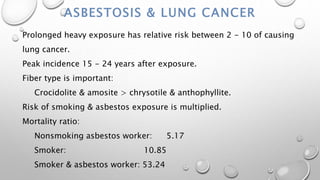
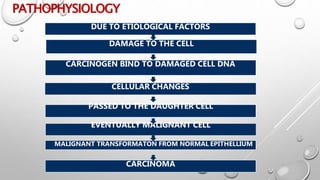
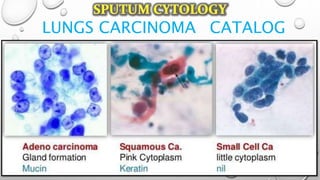
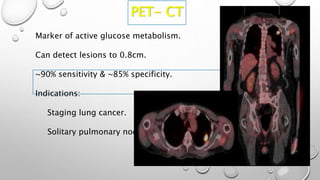
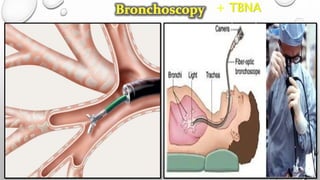

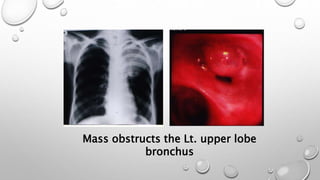
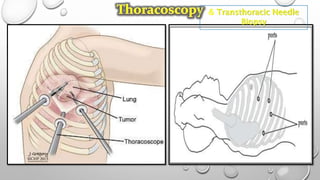

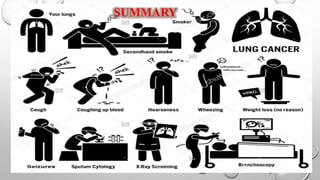

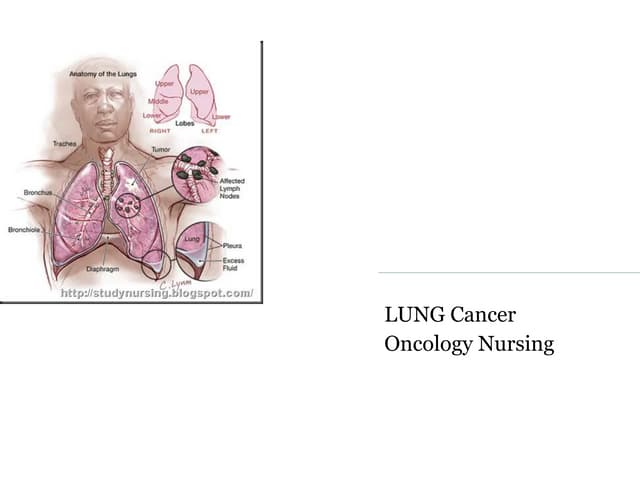
The document discusses lung cancer, its types, risk factors, diagnosis, and treatment options. It describes that lung cancer is uncontrolled cell growth in lung tissues and the major types are small cell lung cancer and non-small cell lung cancer such as adenocarcinoma and squamous cell carcinoma. Risk factors include smoking, occupational exposures, family history, and asbestos exposure. Diagnosis involves tests such as CT scans, PET scans, biopsies, and biomarker analysis. Treatment depends on cancer type and stage but may include surgery, chemotherapy, radiation therapy, targeted therapy, immunotherapy, or a combination.



































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















