Downloaded 183 times















































1) Abdominal trauma is commonly encountered and can be life-threatening. Identification of serious intra-abdominal injuries can be challenging. 2) Motor vehicle accidents account for 60% of abdominal trauma, with blunt trauma more common than penetrating injuries. 3) Injuries to solid organs like the spleen, liver, and kidneys require careful assessment and may be graded based on severity. Conservative management is often attempted initially if the patient is stable. 4) Diagnostic tools like FAST ultrasound, CT scans, and laparoscopy can help identify injuries, but repeated examinations are often necessary. Management may involve surgery or conservative approaches depending on injury severity and patient stability.
Introduction to abdominal trauma, its significance in emergency care, and the challenges in assessment.
Statistics on the occurrence of abdominal trauma, peak incidence age, and global death rates due to injuries.
Different types of abdominal trauma, including blunt and penetrating injuries, and their causes such as accidents and domestic violence.
Focus on rapid transport to trauma centers, airway management, and essential initial care.
Primary survey process, identification of life-threatening conditions, and immediate care practices.
Detailed examination procedures, including systemic surveys and history taking to identify hidden injuries.
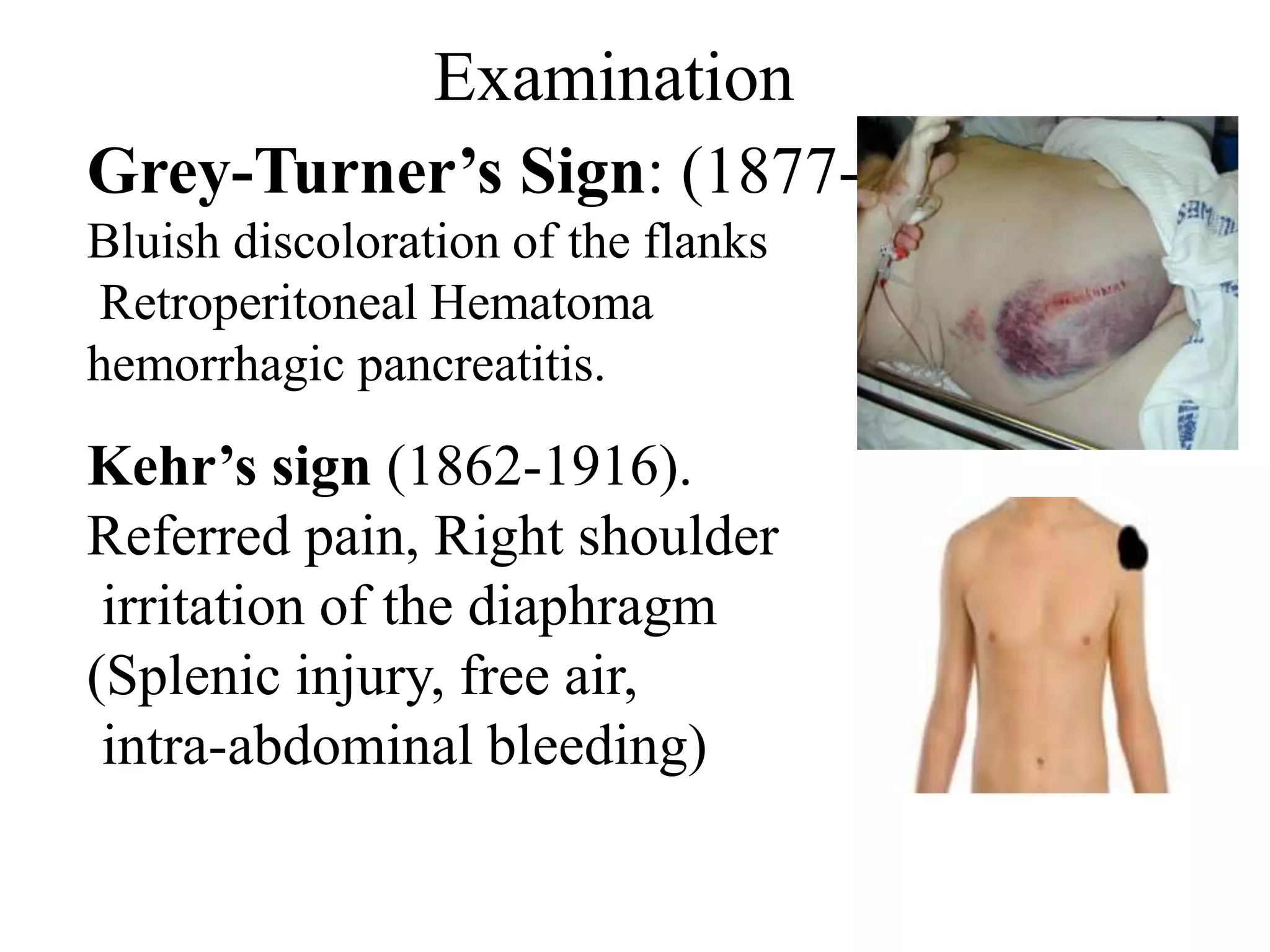
Clinical signs such as Cullen’s sign and Grey-Turner’s sign associated with abdominal trauma.
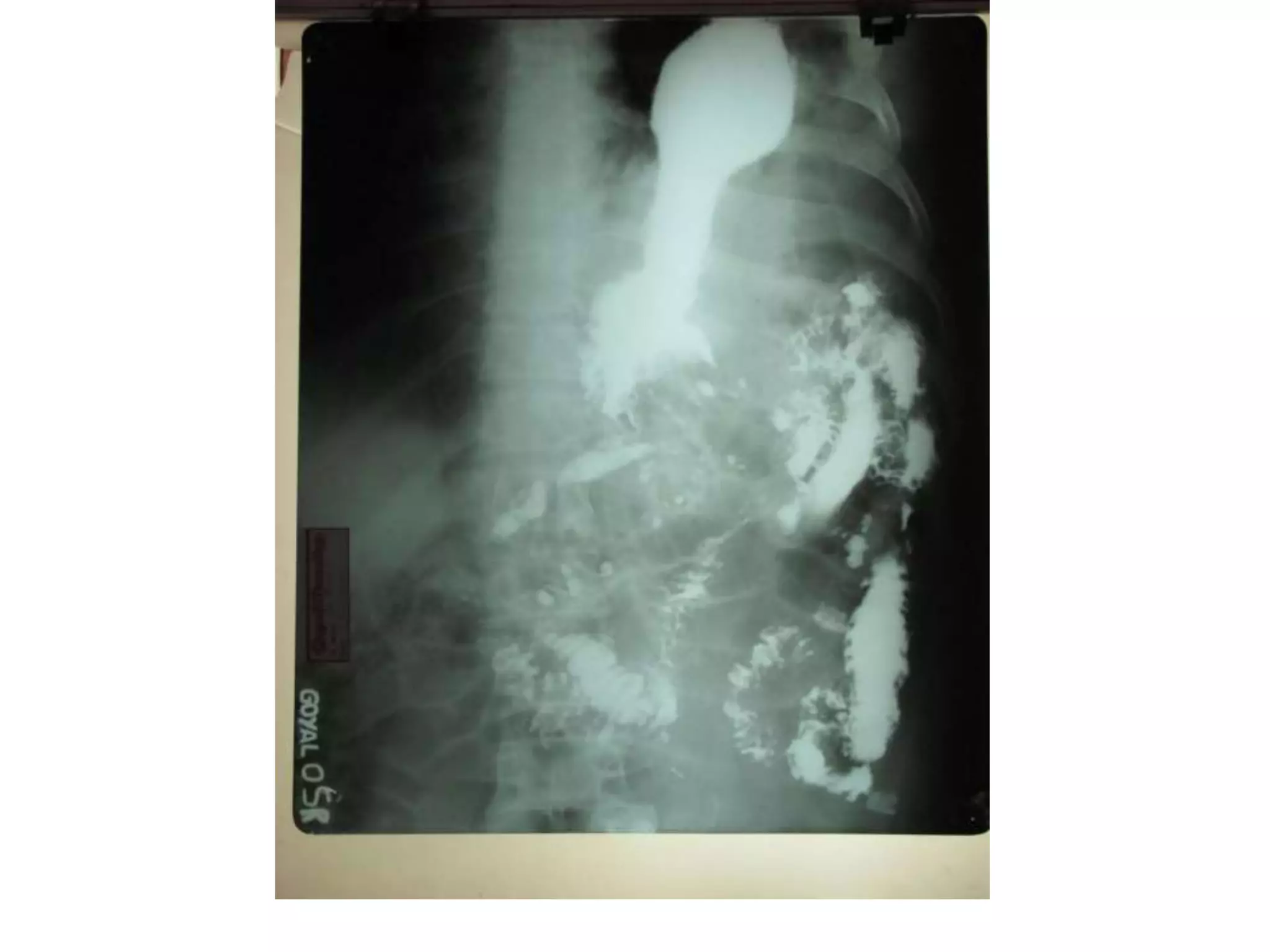
Methods for diagnosing abdominal injuries including FAST, X-Ray, and CT scan, highlighting their effectiveness.
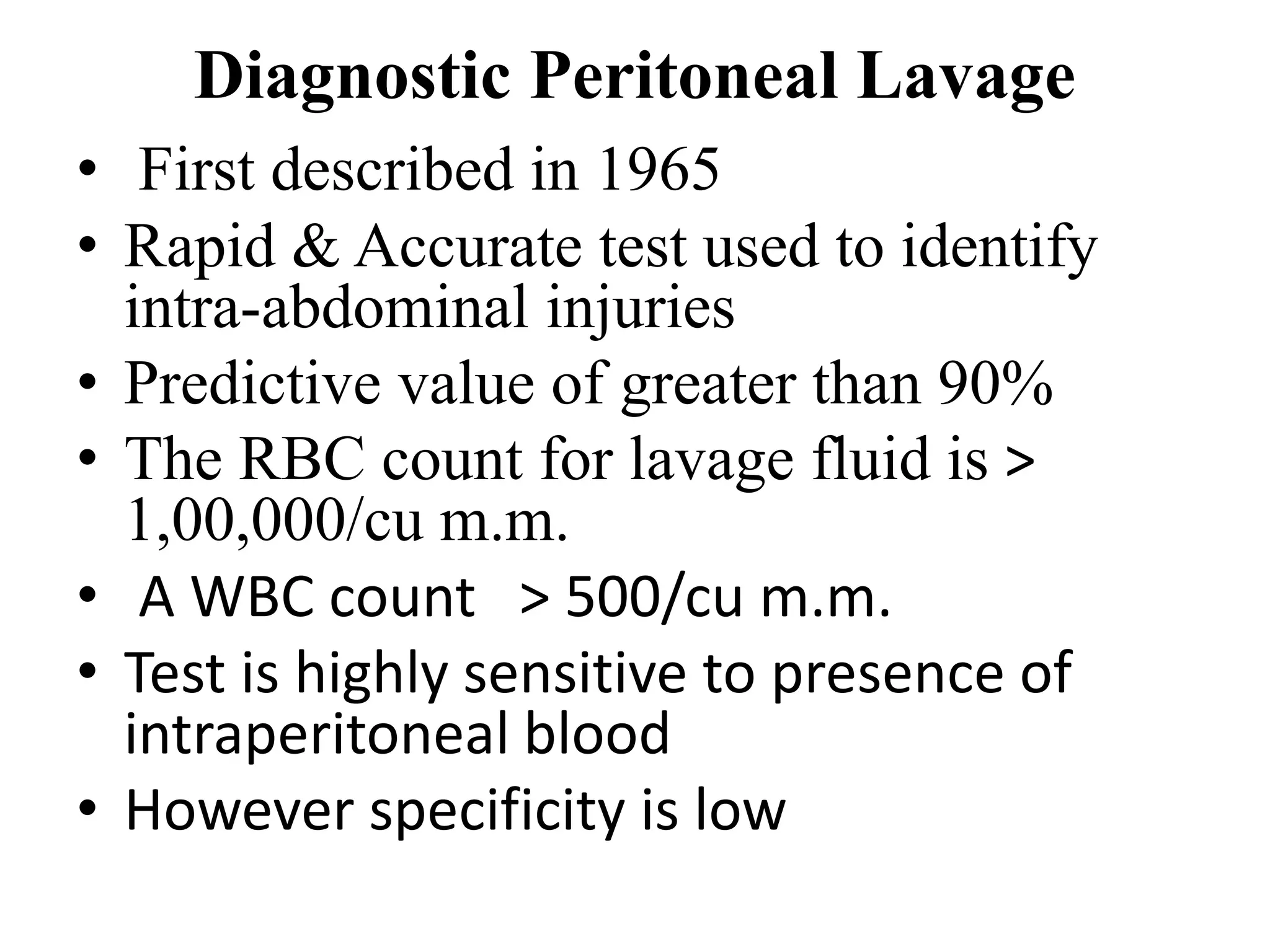
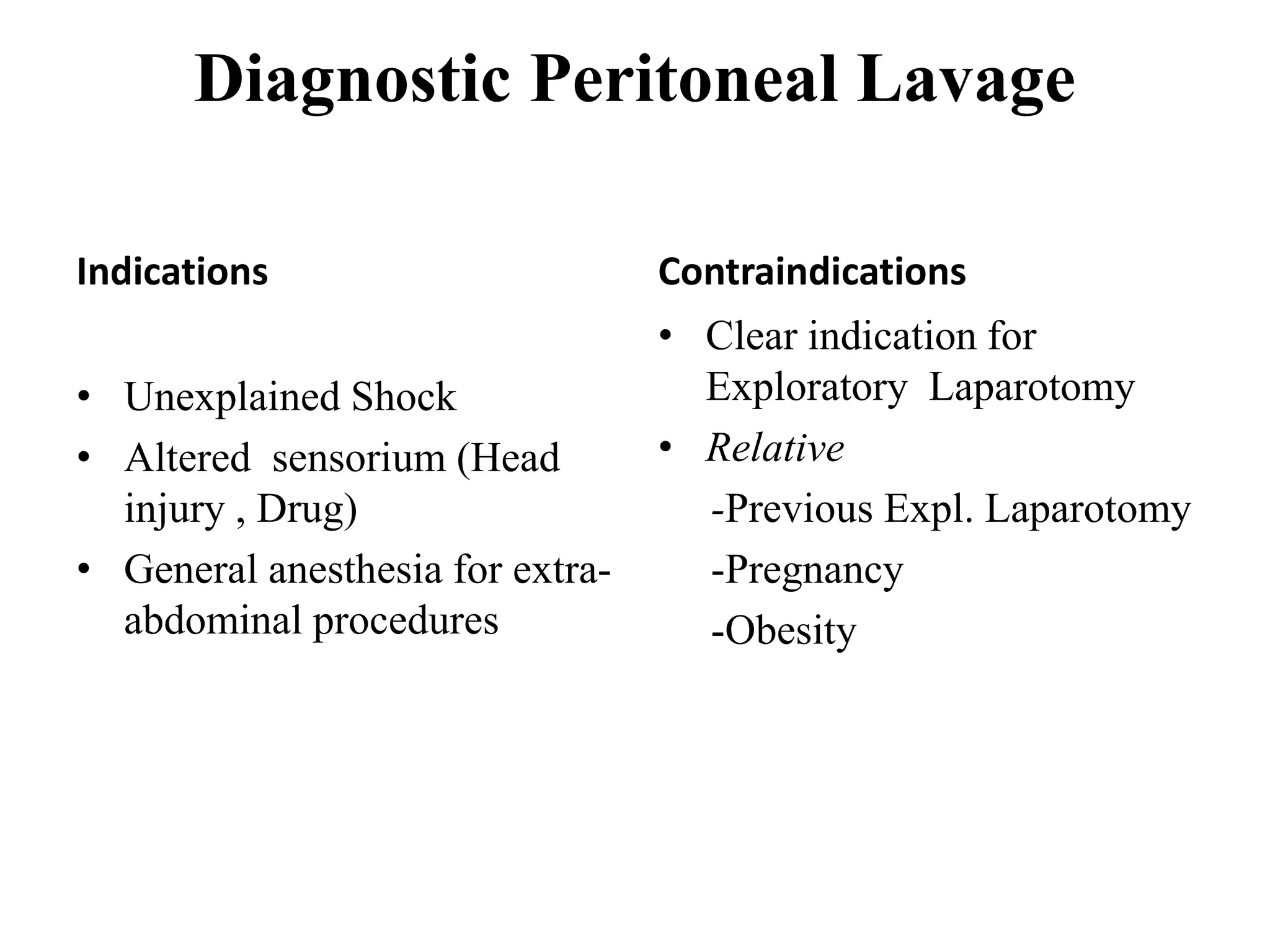
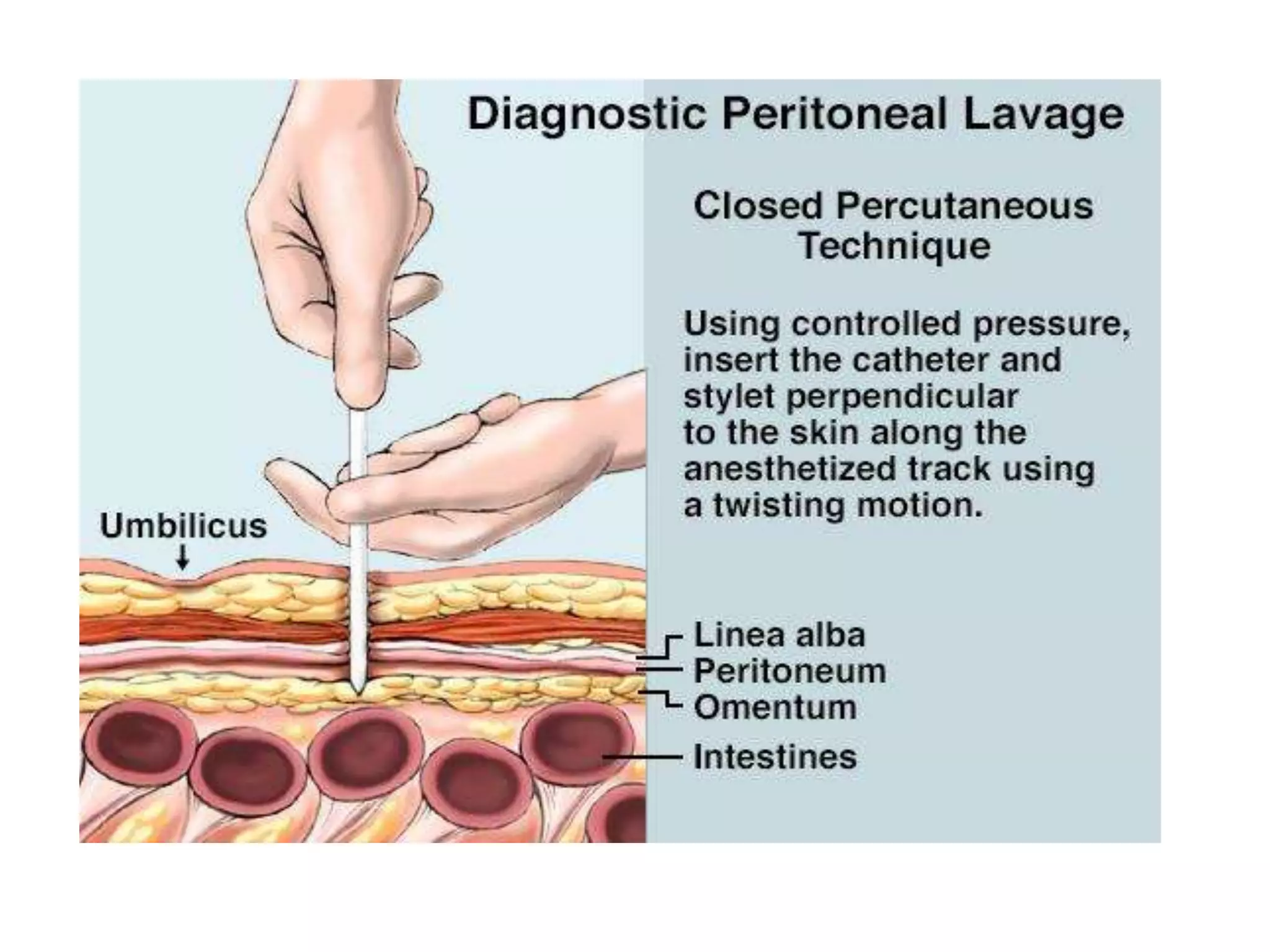
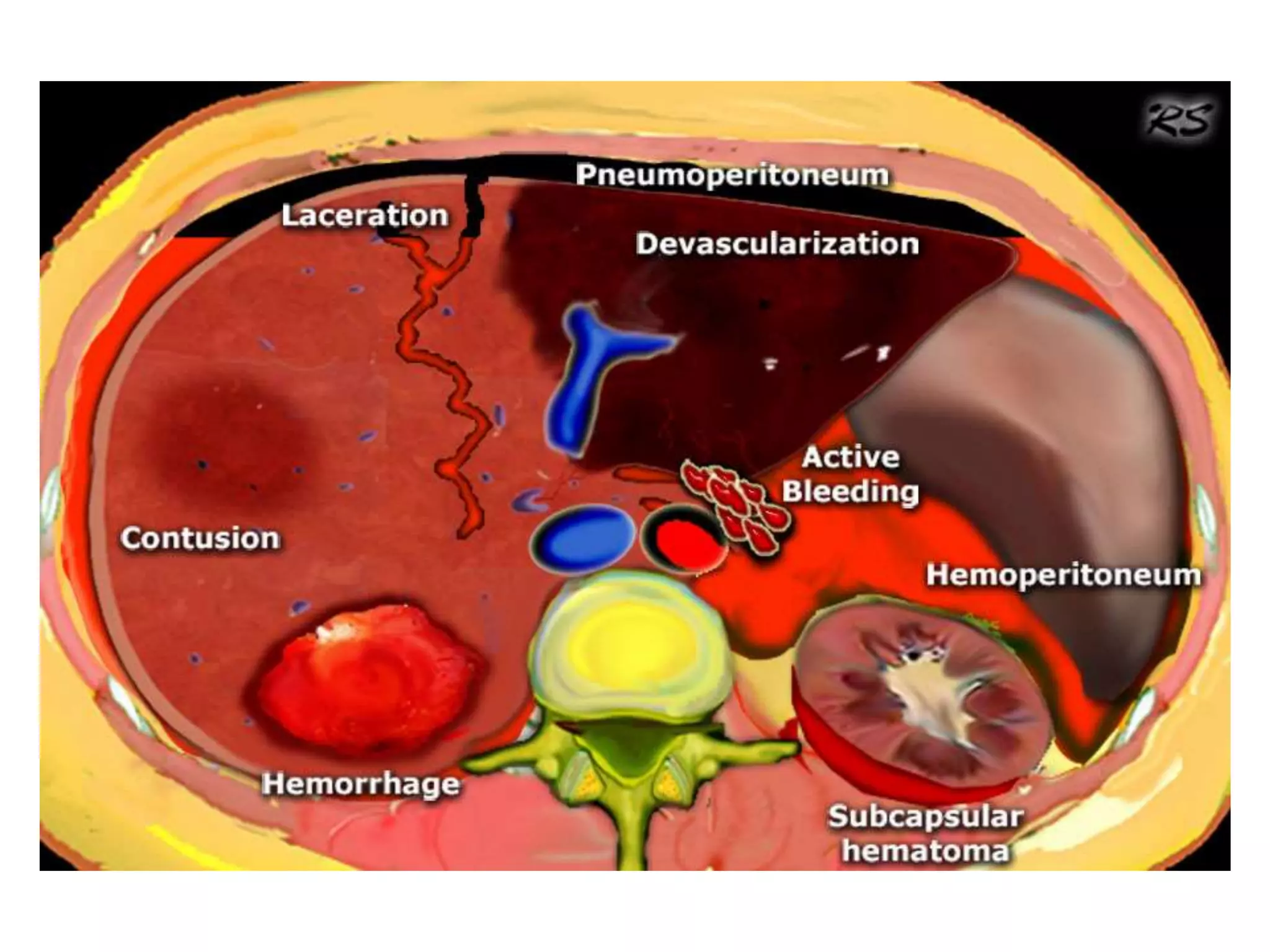
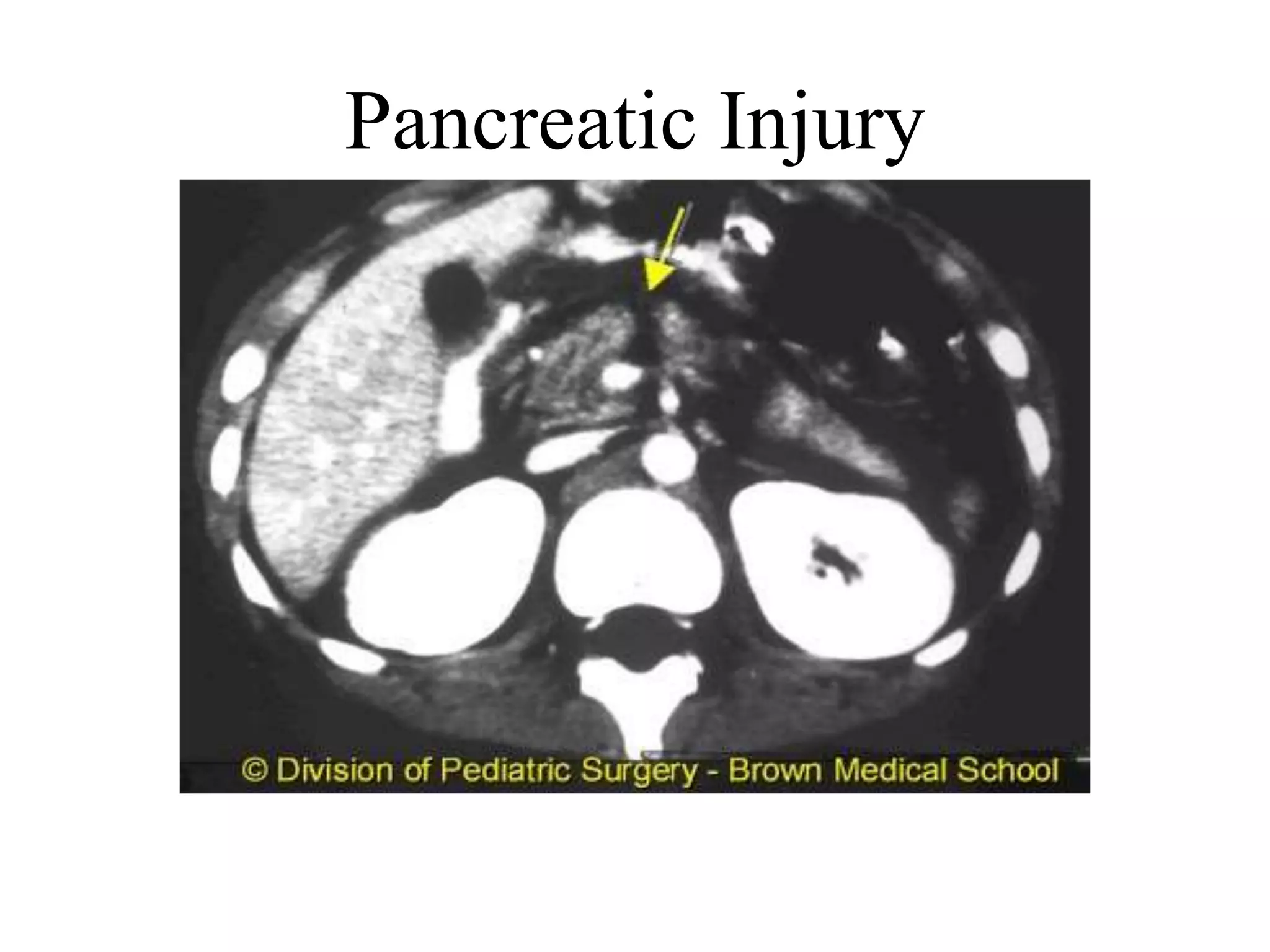
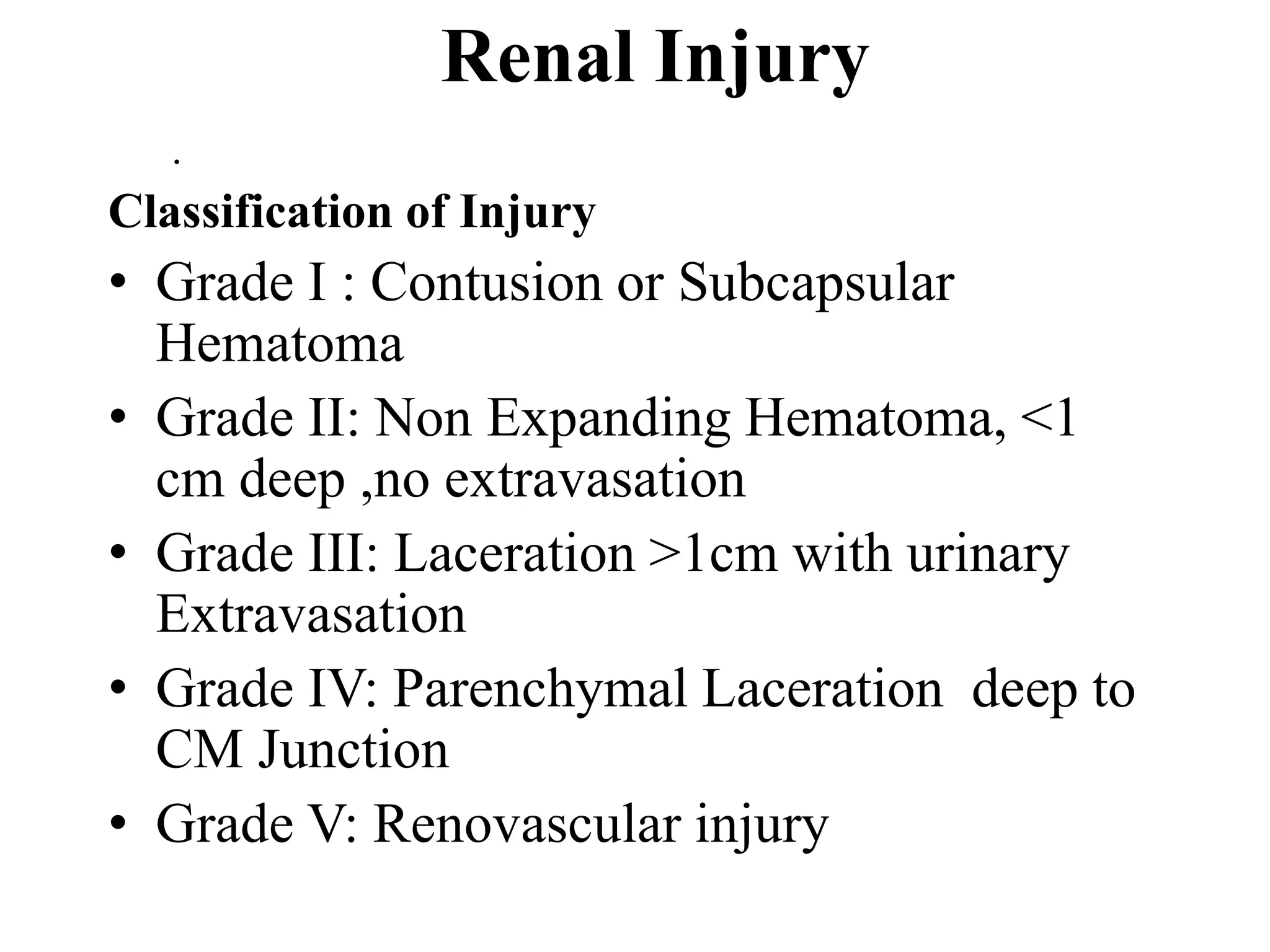
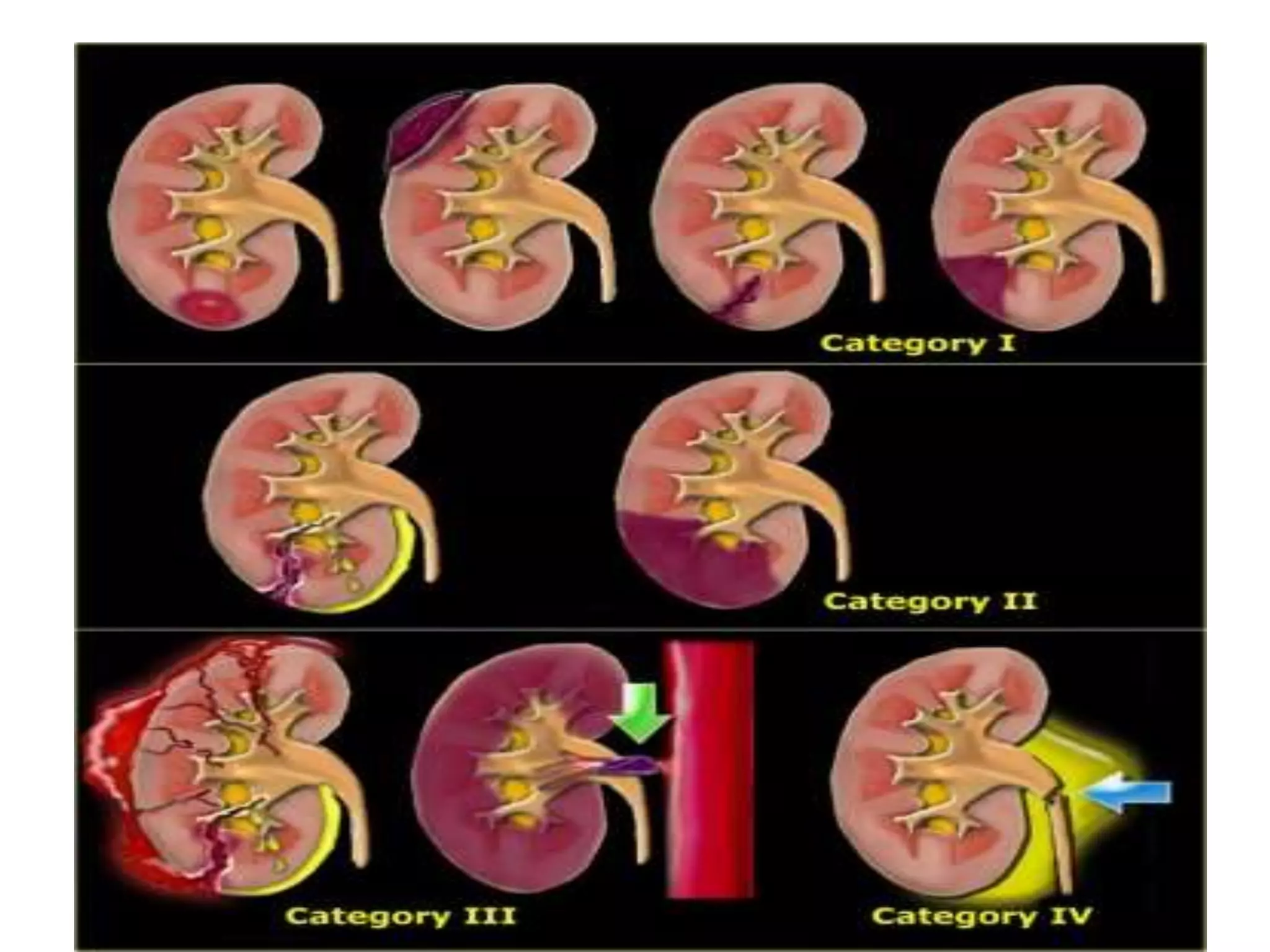
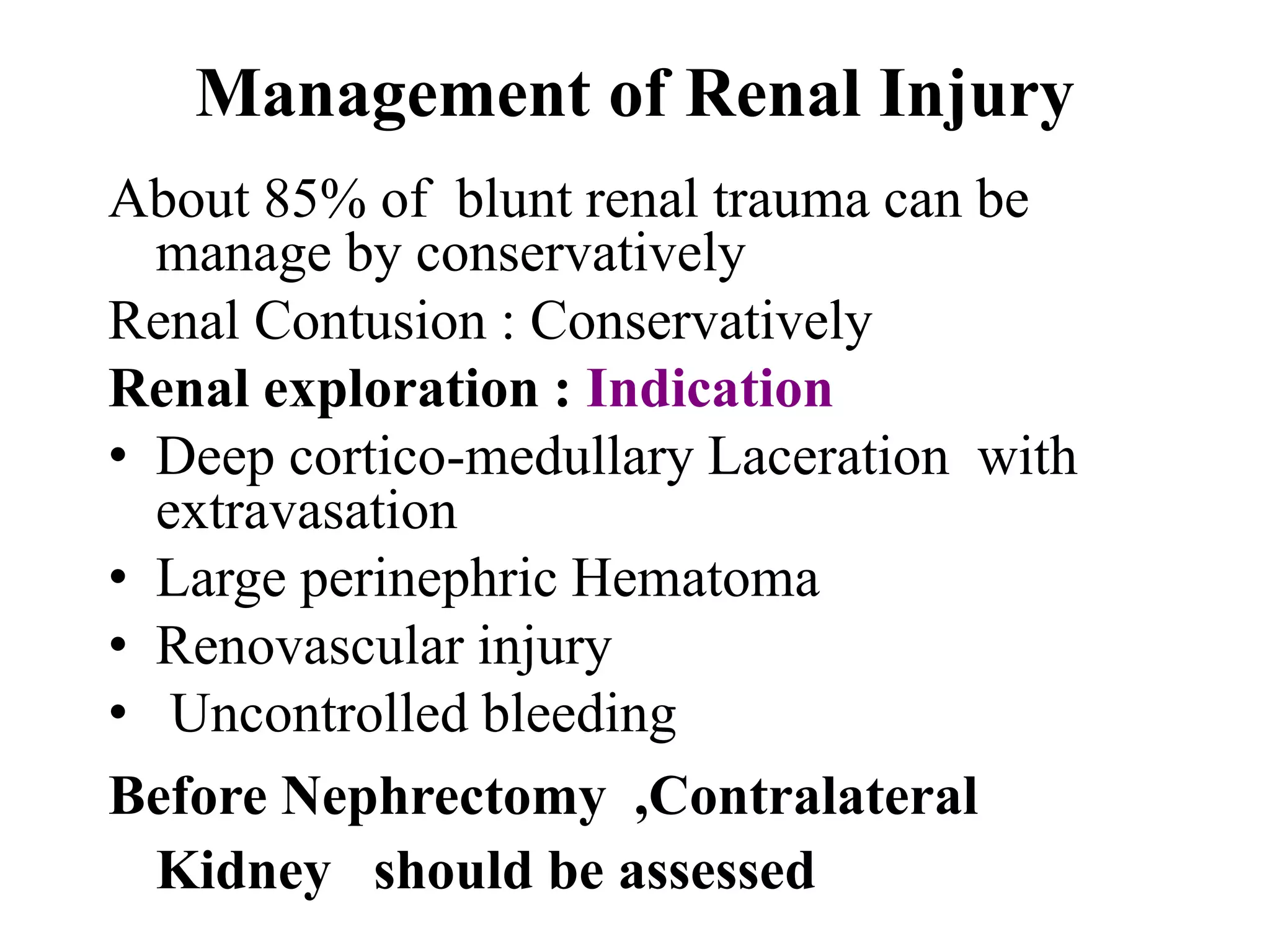
Procedures like paracentesis, diagnostic peritoneal lavage, and the nuances of injuries to solid organs. Injury details focusing on spleen, liver, pancreas, and renal injuries, including diagnosis and management strategies.
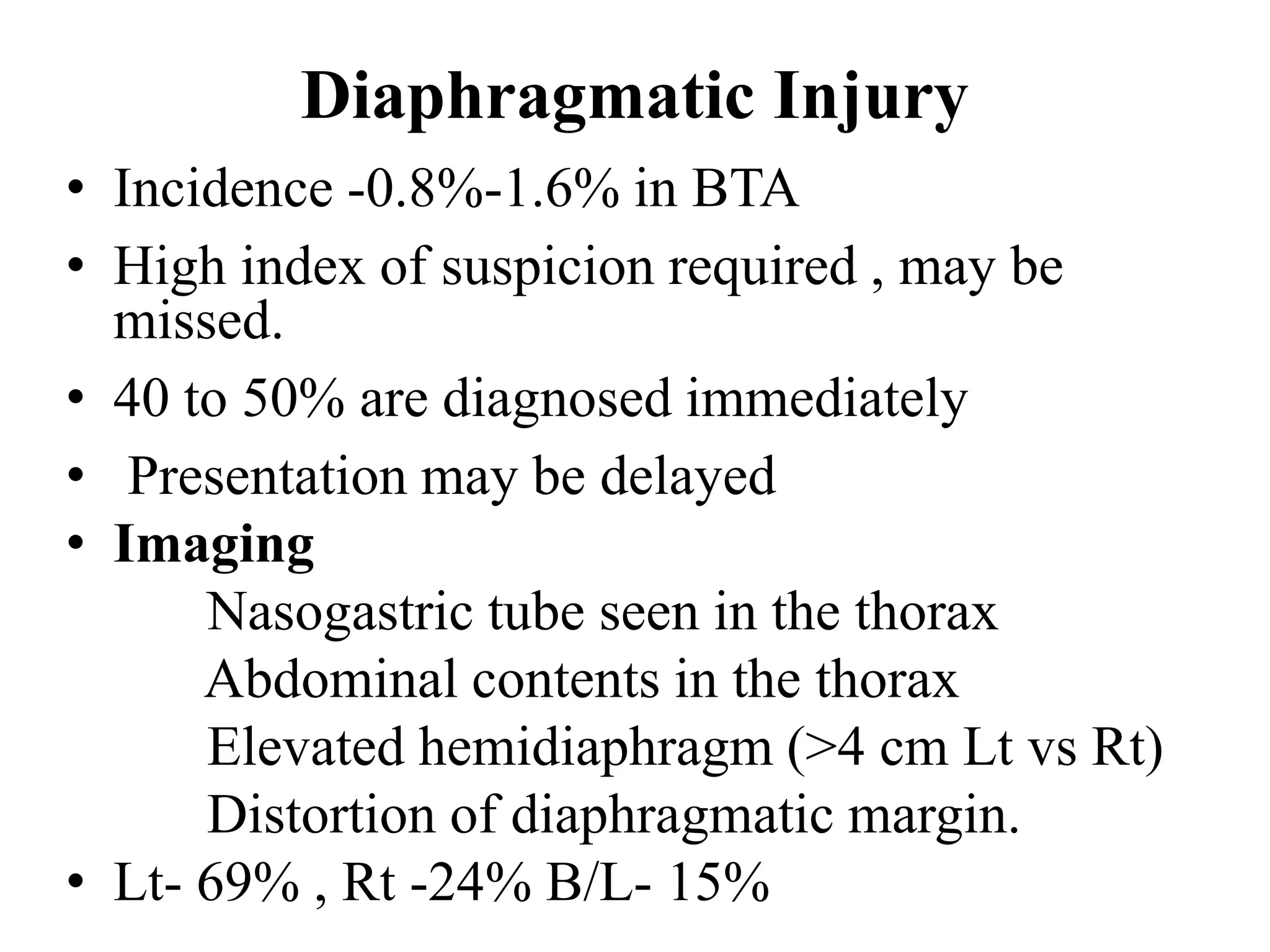
Challenges in diagnosing diaphragm injuries and hollow viscus injuries, including strategies for treatment.
Bladder and ureteral injuries, diagnosis methods, and management practices.
Incidence of trauma in pregnant women, causes, and the multidisciplinary approach needed for management.
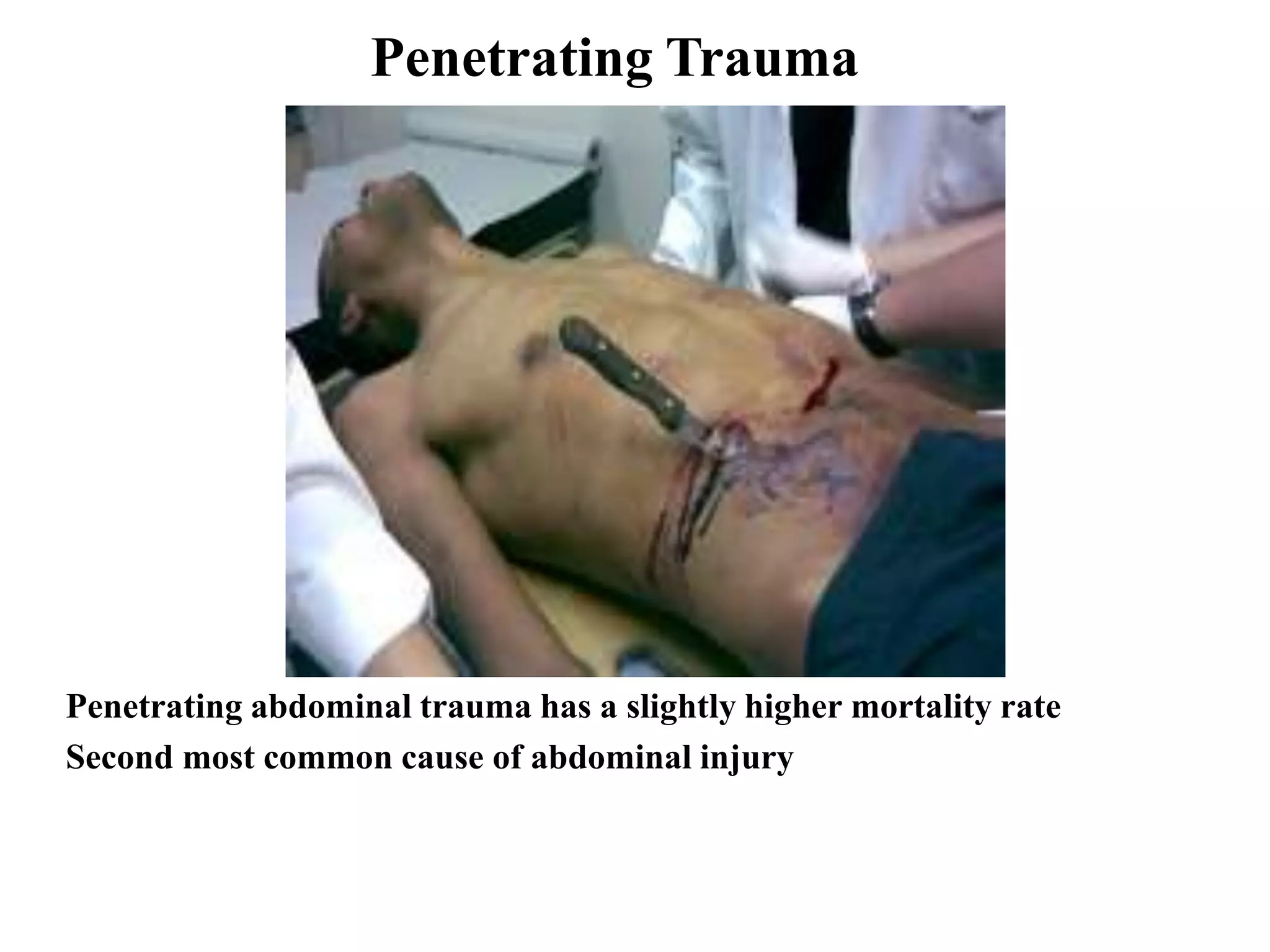
Characteristics of penetrating injuries, specifics about surgery requirements, and associated risks.
Injury prevention strategies focusing on education, safety measures, and statistical impact on injury rates.
Overall insights on injury preventability, trauma health burden, and the importance of integrated care.























































































