Downloaded 63 times
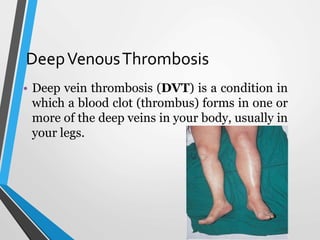
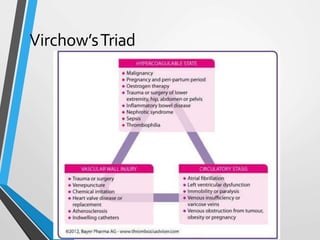

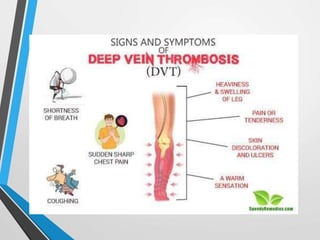

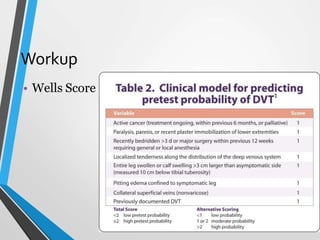

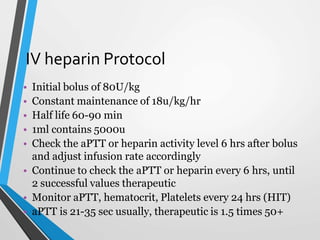
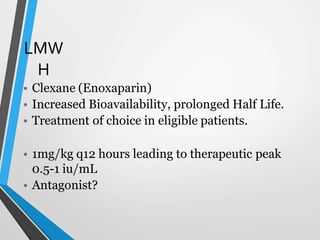
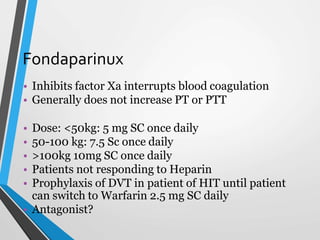
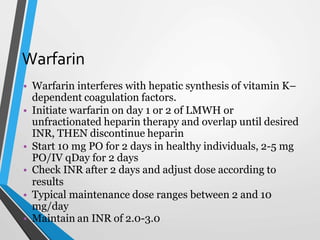
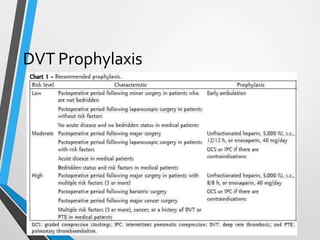
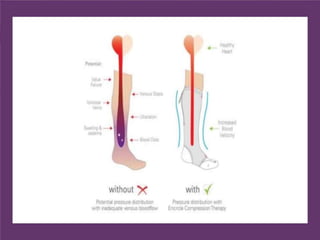

Deep vein thrombosis (DVT) is a blood clot that forms in the deep veins, usually in the legs. Virchow's triad of venous stasis, hypercoagulability, and endothelial injury can lead to thrombus formation. Risk factors include age, immobilization, surgery, cancer, and genetic factors. Patients may experience pain, swelling, warmth, and tenderness. Diagnosis involves a Wells score, D-dimer test, ultrasound or venography. Treatment is anticoagulation with heparin, low molecular weight heparin, fondaparinux, or warfarin to prevent pulmonary embolism. Long-term anticoagulation and compression stockings can help prevent























































































