Downloaded 4,487 times
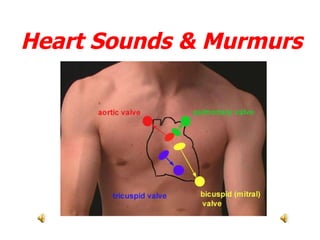
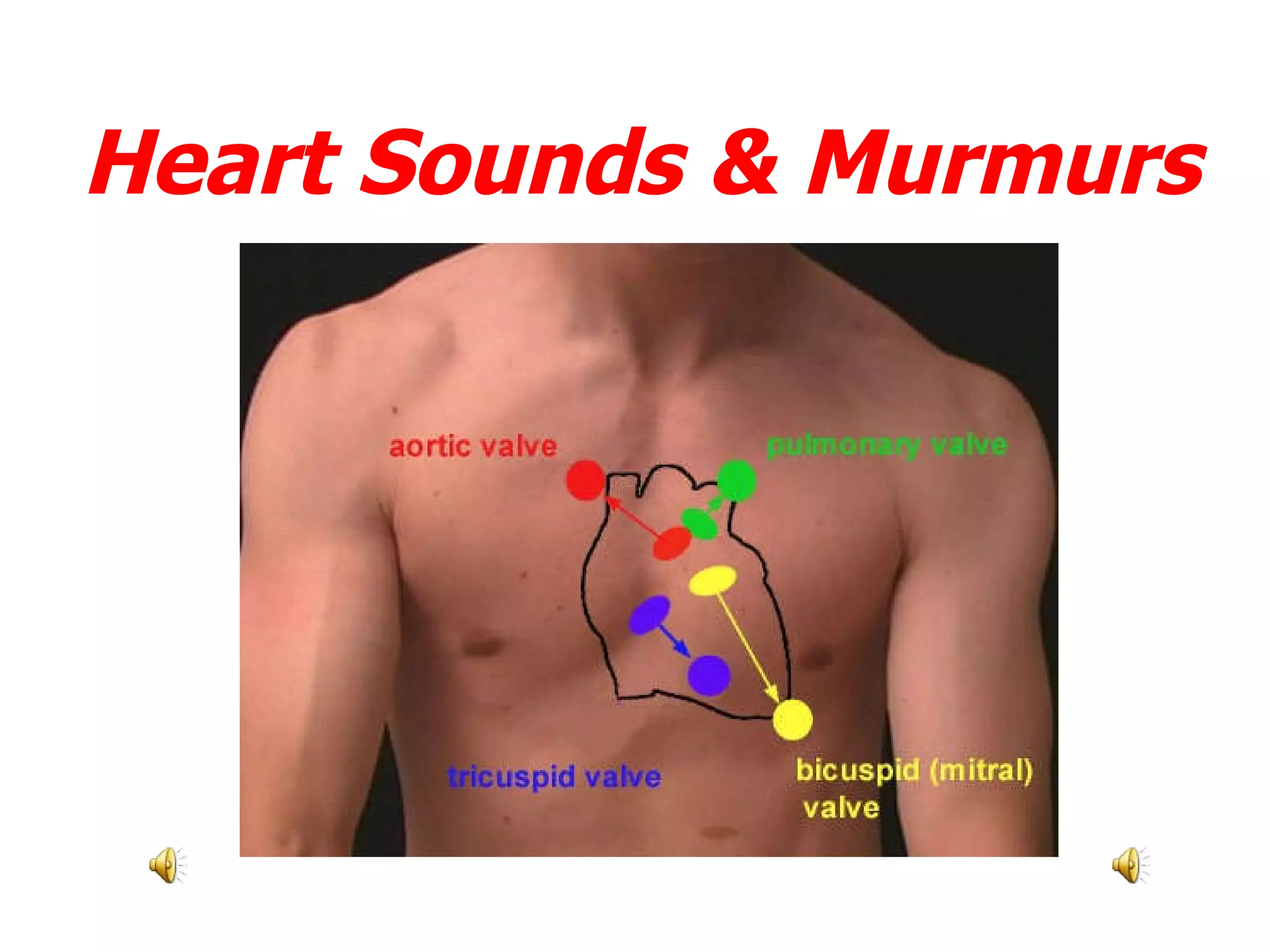
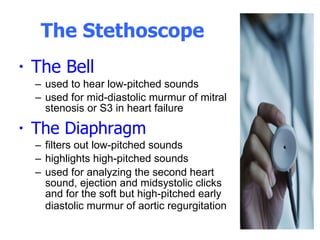
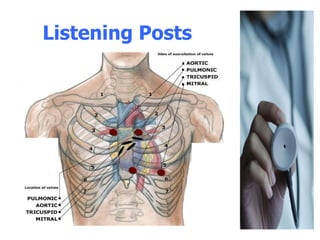
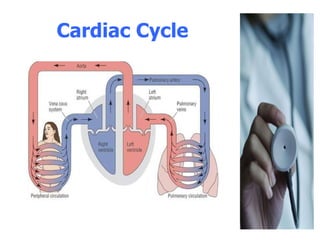
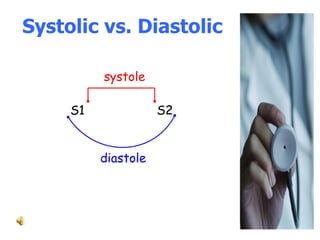
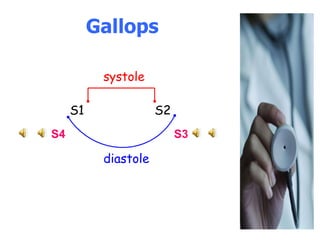

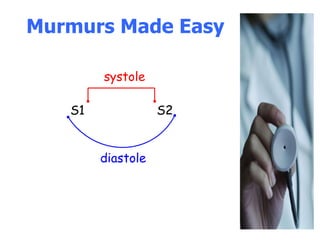
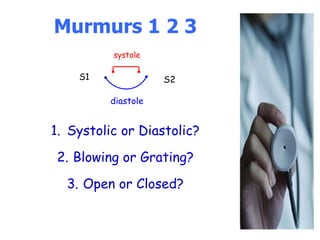
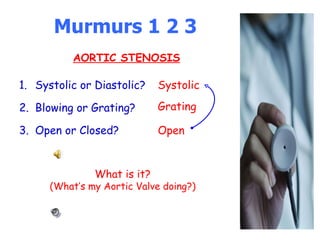
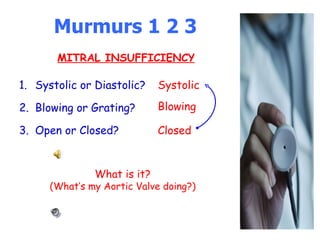



This document provides an overview of heart sounds and murmurs, including how to use a stethoscope to listen to the heart and identify normal and abnormal sounds. It describes the four main heart sounds (S1, S2, S3, S4), their timing in the cardiac cycle, and common causes of extra heart sounds or murmurs such as mitral regurgitation, aortic stenosis, and congestive heart failure. Listening locations are identified for different sounds and murmurs. Characteristics like timing, quality, and radiation are described to help differentiate normal versus pathological findings.

















































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

























































