Downloaded 114 times
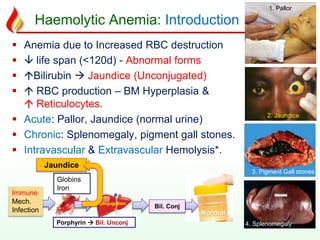
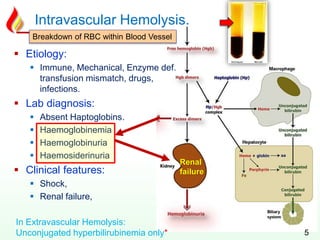
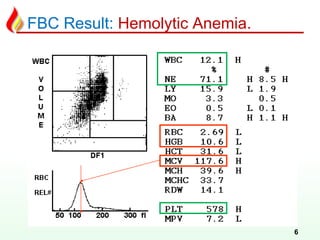
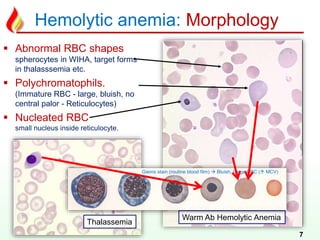
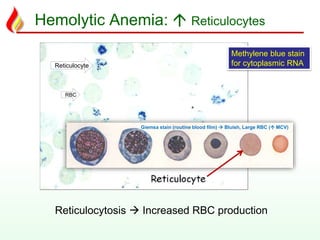
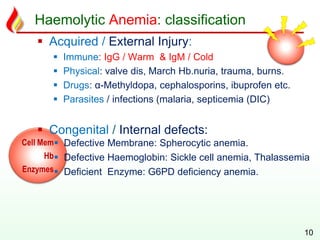
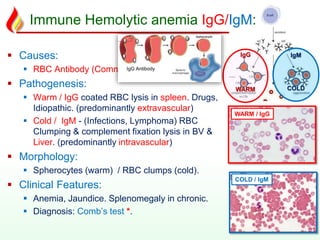
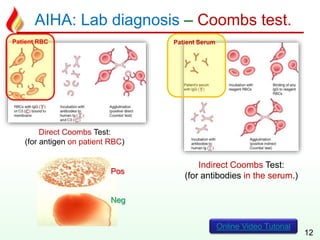
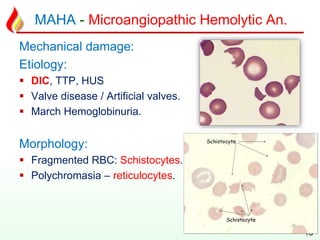


The document discusses hemolytic anemia, its classification, causes, clinical features, and laboratory diagnosis. It emphasizes the importance of understanding both acquired and congenital forms, as well as the typical laboratory findings associated with different types of hemolytic anemia. Additionally, the document includes motivational quotes to encourage a proactive mindset in challenges.