Downloaded 161 times
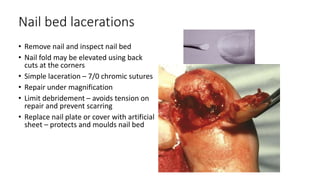
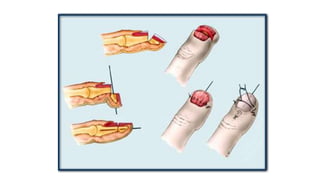

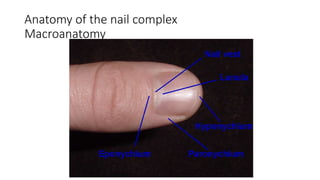












The document discusses nail bed injuries, outlining anatomy, function, and repair techniques. It highlights various types of injuries, their treatments, and emphasizes the importance of careful inspection and management of associated structures. Additionally, it covers advanced repair strategies for complex lacerations and avulsions, addressing complications like nail deformities and loss of nail functionality.











































































































