Downloaded 371 times
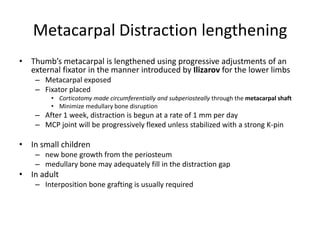
![Metacarpal Distraction lengthening
• Best Indication/Unique Advantages
– Distal subtotal amputation (region of [MCP] joint)
is an indication for this procedure and there is
little or no donor defect except scar.
• Disadvantages and Special Requirements
– Only limited lengthening is possible
– Absolute cooperation is required](https://image.slidesharecdn.com/thumbreconstruction-130515092553-phpapp01/85/Thumb-reconstruction-20-320.jpg)
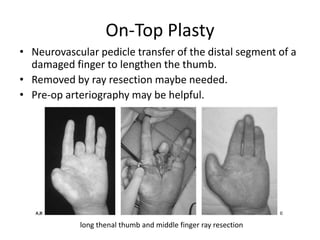
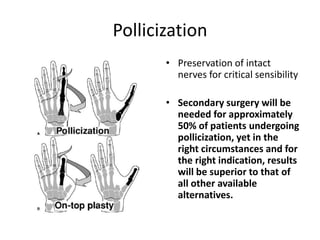

This document discusses various techniques for reconstructing thumb deficiencies caused by trauma or congenital conditions. It describes options for different types and levels of thumb amputation or component loss, including replantation, osteoplastic reconstruction, phalangization, pollicization, toe transfers, and others. Key points covered include indications and disadvantages of each technique, as well as surgical details. Replantation is generally preferred if possible. Other options aim to restore length, stability, and function of the thumb through bone grafting, tendon transfers, and neurovascular repairs or transfers.