Downloaded 121 times

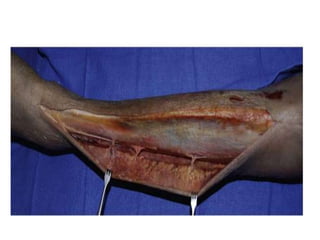
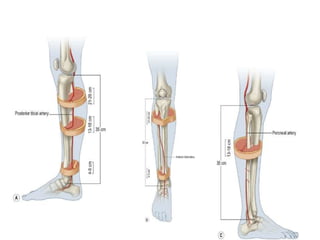
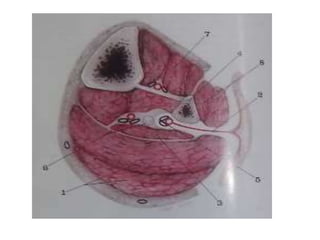







The document discusses the reverse peroneal artery flap technique for reconstructing soft tissue defects around the lower leg, ankle, and foot. It notes that reverse sural flaps have been used before with variable success, while free tissue transfer has improved outcomes in some cases. The technique utilizes skin supplied by the peroneal perforators based on a distally pedicled peroneal artery flap to minimize issues with low perfusion and venous drainage seen in other flaps. The flap is raised in a subfascial plane and perfusion is checked after clamping the peroneal artery to confirm sufficient blood flow.











































































































