Downloaded 96 times




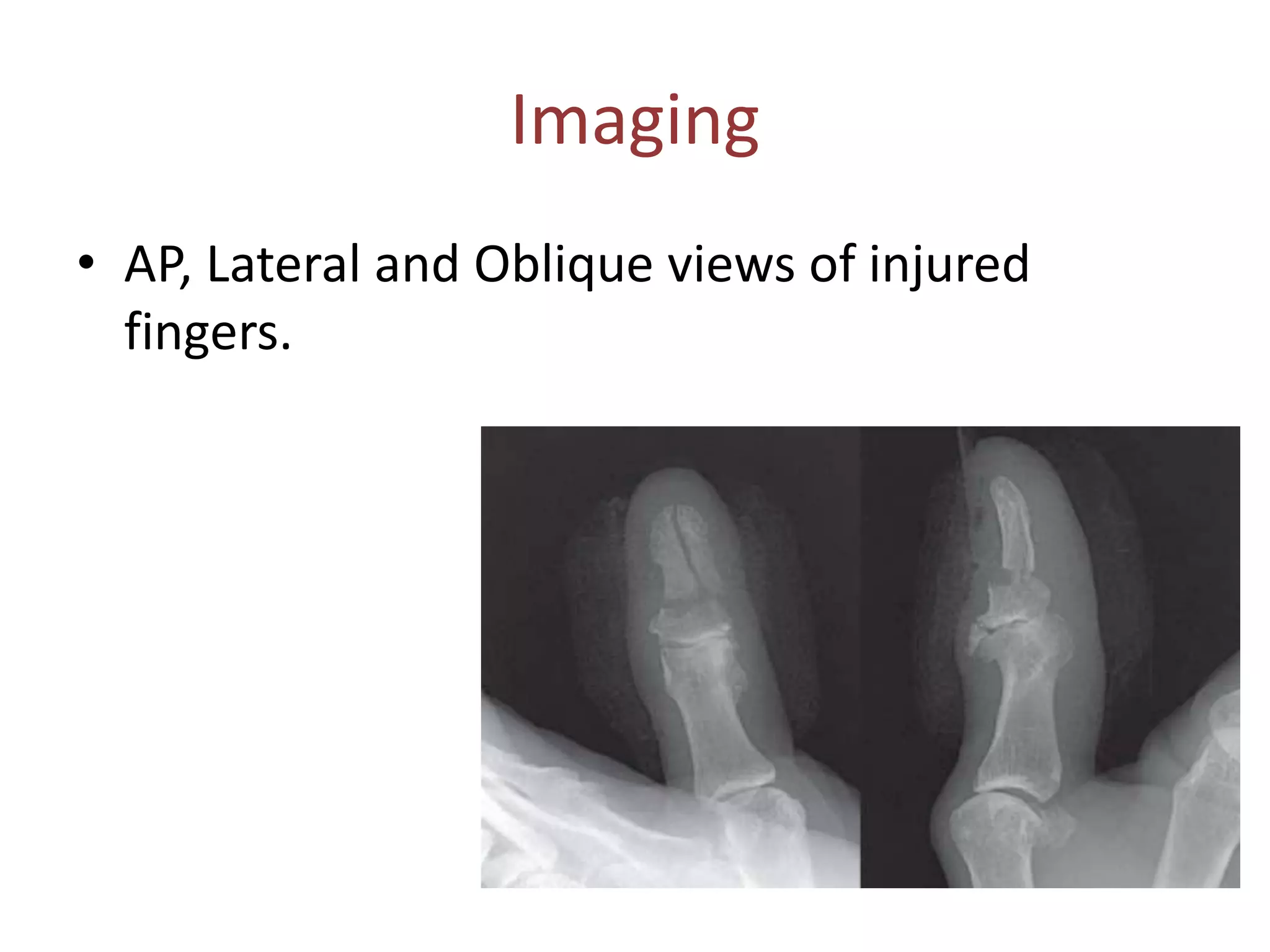





















This document summarizes key information from a seminar presentation on nail bed injuries by Dr. Prajwal K Rao. It discusses the anatomy of the nail unit, causes of nail bed injuries which commonly involve long fingers in males aged 4-30. Clinical examination involves sensory and pattern evaluation as well as matrix involvement. Imaging can include x-rays. Injuries are classified and trephination may help reduce pain. Nail bed repair indications and techniques are outlined, including options when the nail is unavailable. Post-operative care and potential complications are also summarized.



































































