FDMA FLAP - The first dorsal metacarpal artery (FDMA) flap is used mainly for reconstruction of thumb defects
•Download as PPTX, PDF•
0 likes•20 views

Also see the Dr Vinita puri & Dr Nilesh SHENDE Paper First Dorsal Metacarpal Artery Flap a Workhorse for Reconstruction of Selected Small Defects of the Hand Turkish Journal of Plastic Surgery 27(3):p 98-103, Jul–Sep 2019. | DOI: 10.4103/tjps.tjps_71_18

Recommended
More Related Content
Similar to FDMA FLAP - The first dorsal metacarpal artery (FDMA) flap is used mainly for reconstruction of thumb defects
Similar to FDMA FLAP - The first dorsal metacarpal artery (FDMA) flap is used mainly for reconstruction of thumb defects (20)
More from Shubhanshu Gaurav
More from Shubhanshu Gaurav (11)
Recently uploaded
Recently uploaded (20)
FDMA FLAP - The first dorsal metacarpal artery (FDMA) flap is used mainly for reconstruction of thumb defects
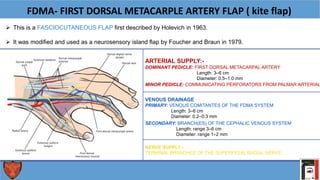
- 1. FDMA- FIRST DORSAL METACARPLE ARTERY FLAP ( kite flap) This is a FASCIOCUTANEOUS FLAP first described by Holevich in 1963. It was modified and used as a neurosensory island flap by Foucher and Braun in 1979. NERVE SUPPLY:- TERMINAL BRANCHES OF THE SUPERFICIAL RADIAL NERVE ARTERIAL SUPPLY:- DOMINANT PEDICLE: FIRST DORSAL METACARPAL ARTERY Length: 3–6 cm Diameter: 0.5–1.0 mm SECONDARY: BRANCH(ES) OF THE CEPHALIC VENOUS SYSTEM Length: range 3–6 cm Diameter: range 1–2 mm MINOR PEDICLE: COMMUNICATING PERFORATORS FROM PALMAR ARTERIAL VENOUS DRAINAGE PRIMARY: VENOUS COMITANTES OF THE FDMA SYSTEM Length: 3–6 cm Diameter: 0.2–0.3 mm
- 2. FLAP DIMENSIONS Length: 3 cm (range 2–5 cm) Width: 2 cm (range 1.5–3 cm) Thickness: the thickness of the dorsum of the hand FLAP COMPONENTS: SKIN AND SUBCUTANEOUS TISSUE ARC OF ROTATION FOR DORSAL DEFECT FOR VOLAR DEFECT
- 3. INDICATIONS:- For resurfacing either volar or dorsal defects of the distal thumb as far distal as the interphalangeal (IP) joint. It can be used to cover the ulnar surface of the dorsum of the hand and the wrist, or the palm up to the third metacarpal. It is useful for first web space reconstruction following contracture, and it can provide soft-tissue coverage of the index finger up to the level of the proximal phalanx. There are no specific age restrictions provided that the radial artery is not involved with atheroma. It can be used in both acute trauma and elective reconstruction. CONTRAINDICATIONS:- A radial artery injury in the anatomical snuffbox.
- 4. TECHNIQUE OF HARVEST PREOPERATIVE EXAMINATIONS AND MARKINGS Preoperative Doppler examination for the presence of vessels is mandatory mark the course of the vessels on the skin, because they are always located more radially than presumed PATIENT POSITION Supine with arm on arm table + tourniquet use during harvest DISSECTION Incise skin along the markings along the second metacarpal incise the interosseous muscle fascia preserve the intermuscular septum and raise the fasciocutaneous flap, including the fascia take care to include the nerve and create a de-epithelialized pedicle leave approximately 0.5–1 cm of fatty tissue around the artery preserve the paratenon above the extensor hood open the tourniquet and check for perfusion inset the flap at the recipient site and wait for normal perfusion to occur treat the skin graft donor site with a medium- or full-thickness skin graft be careful when tunnelling.
- 5. THANK YOU.