Downloaded 977 times






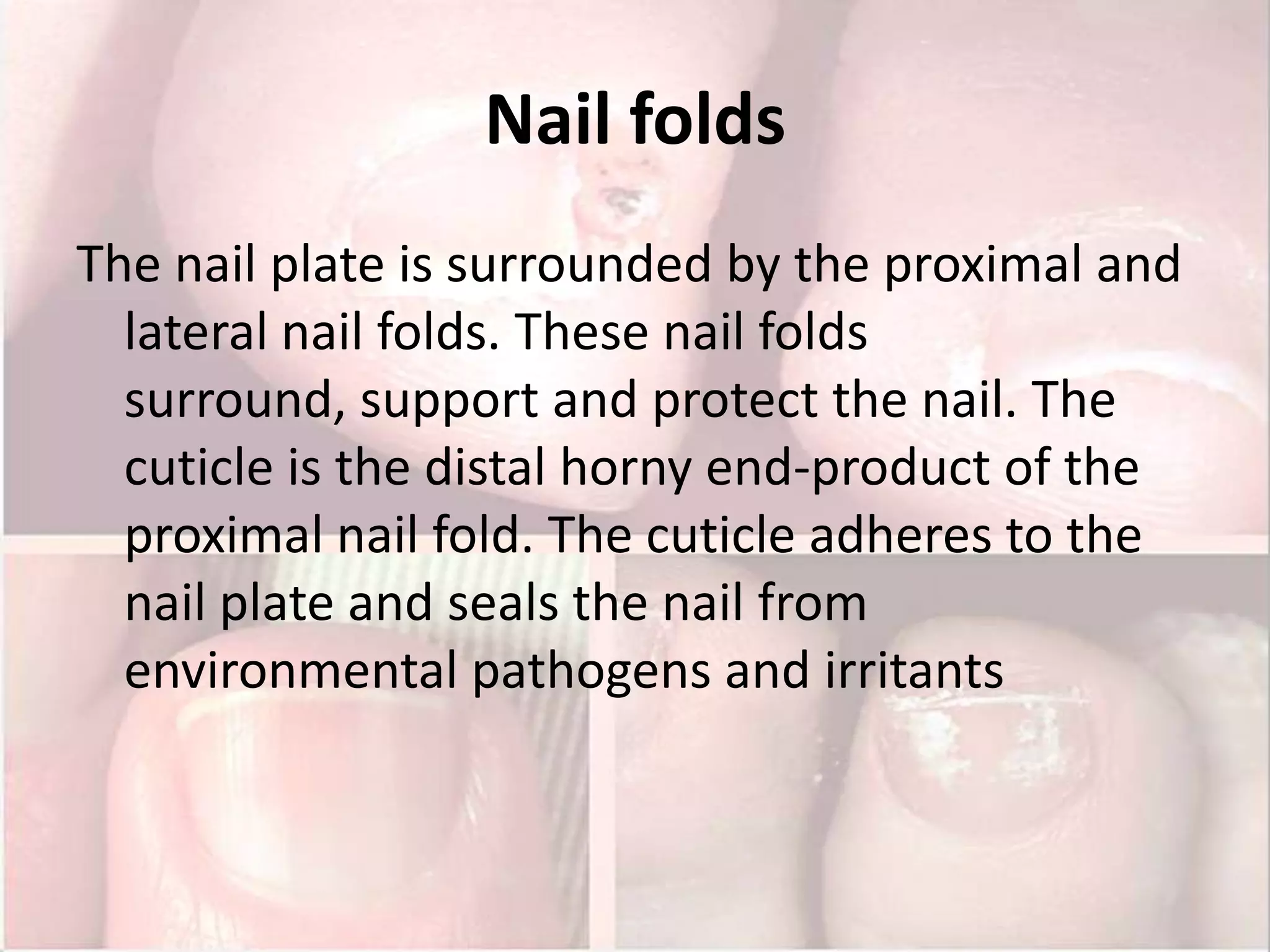
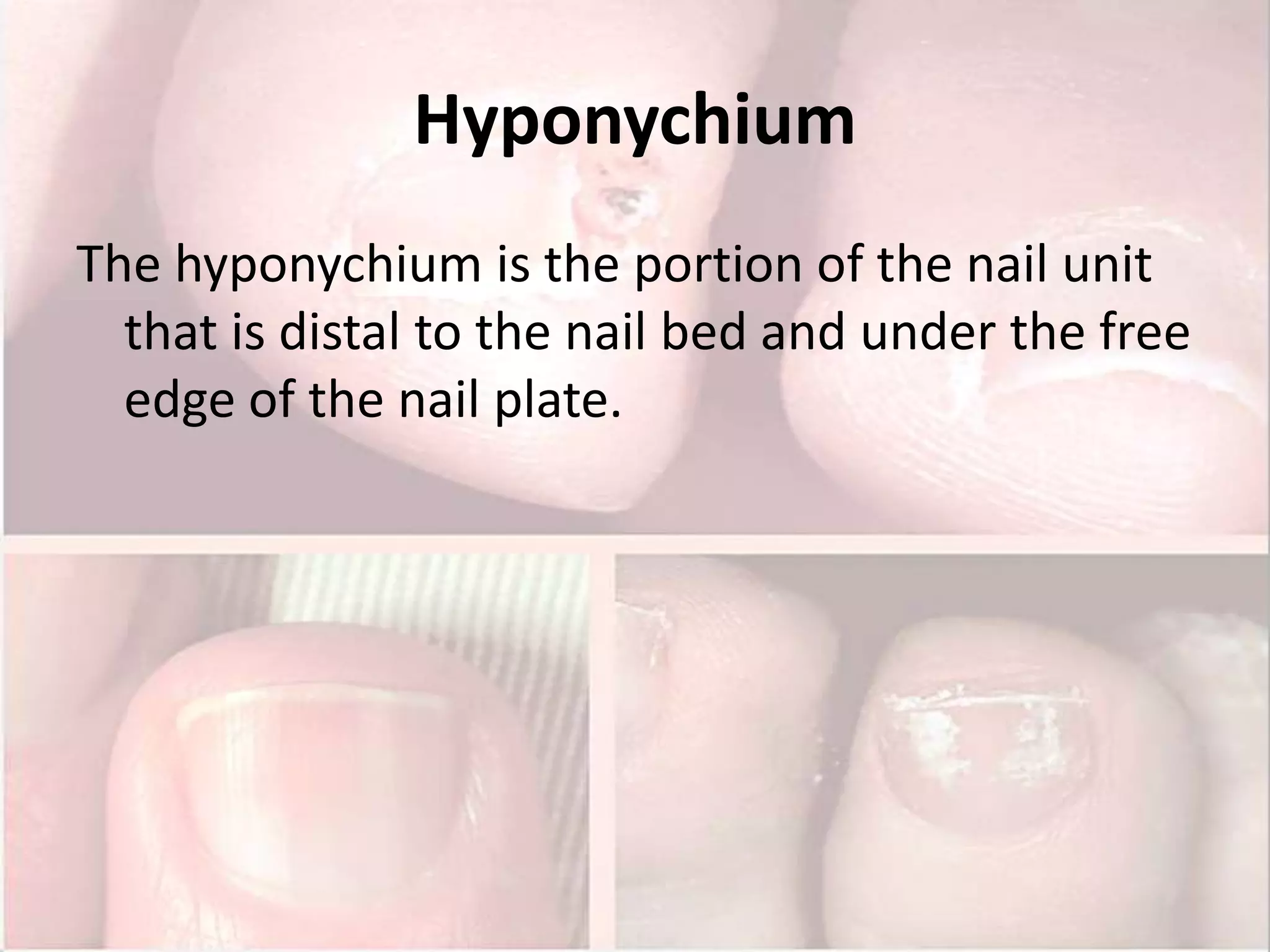




























The document discusses diseases of the nail. It begins by describing nail anatomy including the nail matrix, nail bed, hyponychium, and nail folds. It then discusses examination of nail conditions including history, symptoms, medical history, and lab/imaging workup. Specific nail signs caused by various conditions are defined such as Beau's lines, clubbing, and onychomycosis. Common infectious causes of nail disorders including fungal, bacterial, and viral infections are outlined.























































































