Downloaded 15 times
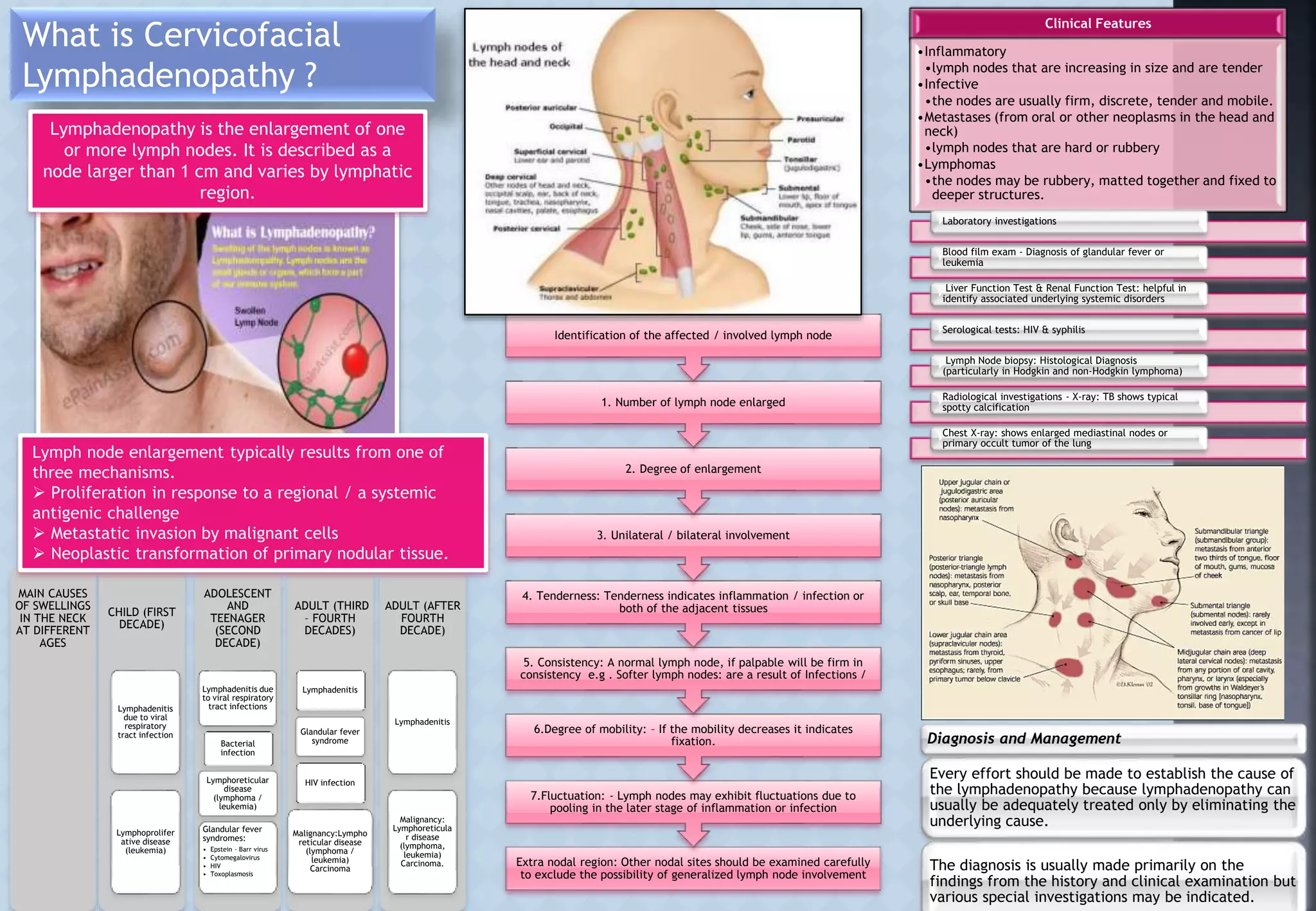

Cervicofacial lymphadenopathy refers to the enlargement of lymph nodes in the neck region. The document outlines several key factors to examine when evaluating enlarged lymph nodes, including their number, size, consistency, tenderness, and mobility. It also discusses the most common causes of neck lymph node swelling at different ages, which can include infections, autoimmune diseases, cancers, and more. Establishing the underlying cause of the lymphadenopathy is important for determining the proper diagnosis and management.



































































