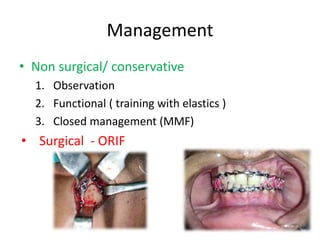
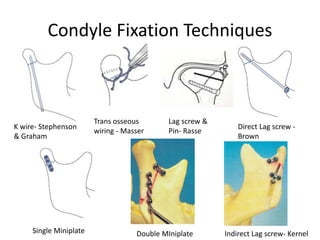
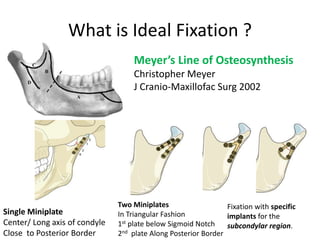
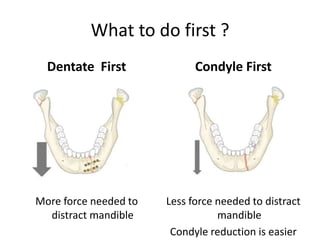
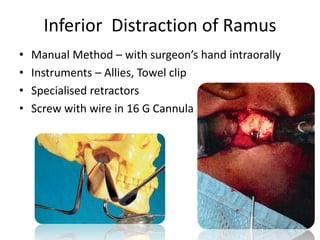
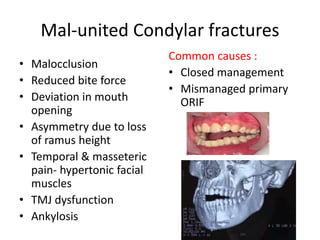
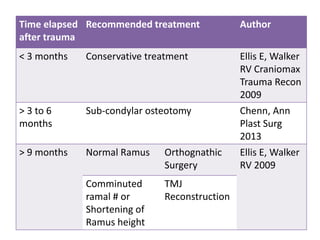
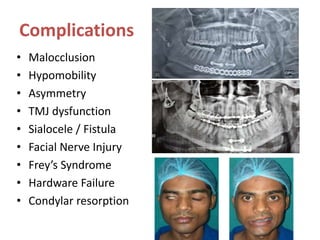
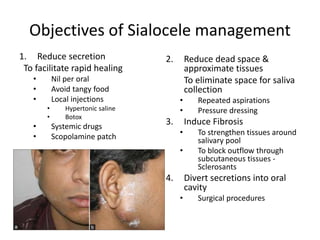
The seminar presented by Dr. Mehul Shashikant Hirani covers condylar fractures, including their anatomy, classification, mechanisms of injury, and management options. It discusses various surgical and non-surgical approaches to treatment, emphasizing the importance of achieving stable occlusion and minimizing complications. Surgical considerations include different approaches and fixation techniques for addressing fractures effectively.