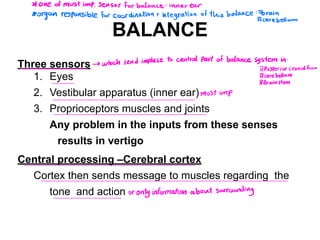
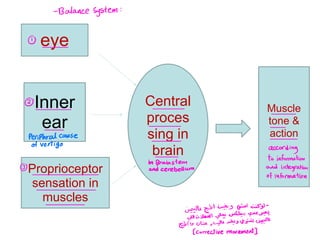
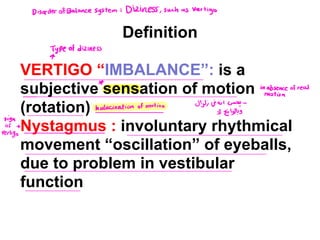
1. The balance system involves three sensors - the eyes, vestibular apparatus in the inner ear, and proprioceptors in muscles and joints. Any problem with these results in vertigo.
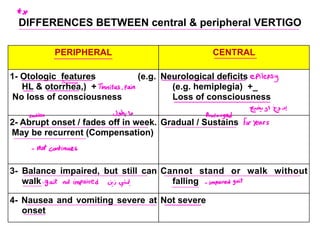
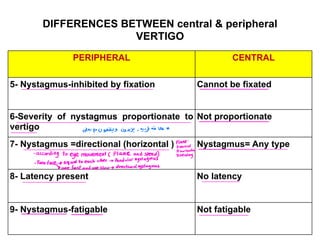
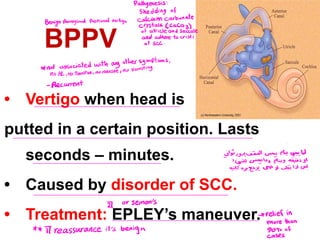
2. Vertigo is caused by issues in the peripheral vestibular system (inner ear or vestibular nerve) or central problems in the brainstem or cerebellum. Common peripheral causes include Meniere's disease, BPPV, and vestibular neuronitis.
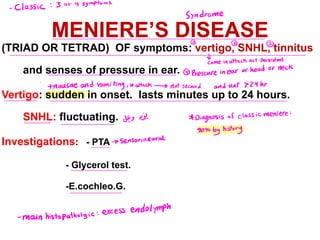
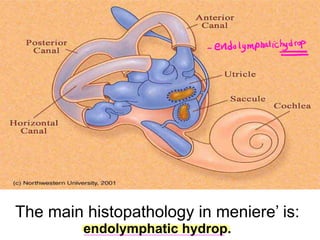
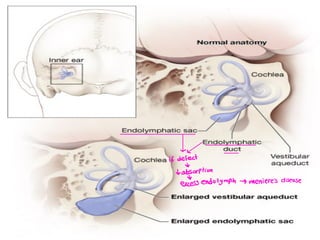
3. Meniere's disease is characterized by the classic triad or tetrad of vertigo, fluctuating sensorineural hearing loss, tinnitus, and a feeling of ear fullness. It is caused by