Downloaded 16 times








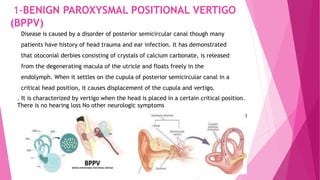
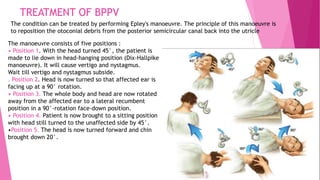

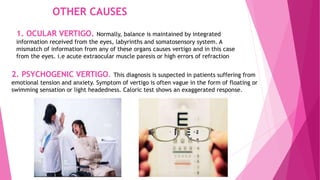






The document discusses tinnitus and vertigo, including their definitions, classifications, causes, and treatment options. Tinnitus is characterized by ringing or noise in the ears, while vertigo is a sensation of spinning, attributed to peripheral or central vestibular disorders. Treatment approaches focus on addressing underlying causes and may include reassurance, psychotherapy, and specific maneuvers for conditions like benign paroxysmal positional vertigo (BPPV).

















































![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)











![Down syndrome (2)[1].pptx pediatric lecture](https://cdn.slidesharecdn.com/ss_thumbnails/downsyndrome21-240709094926-fcdd02d9-thumbnail.jpg?width=640&height=640&fit=bounds)

























