Downloaded 68 times


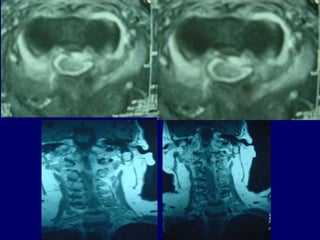

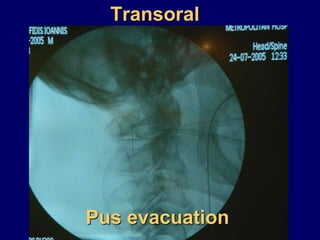
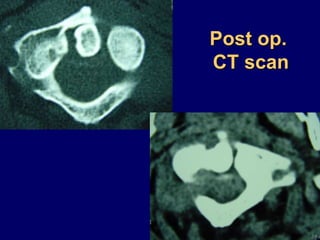
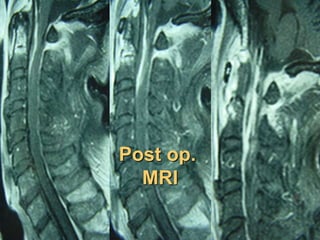



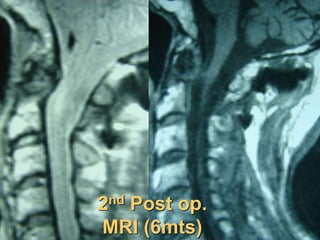


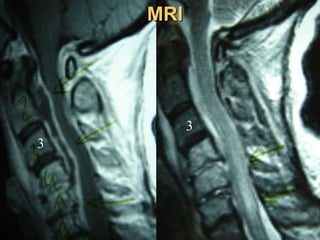
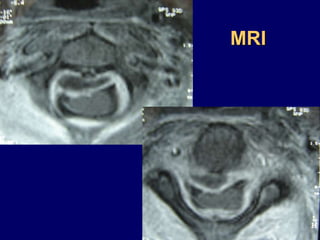
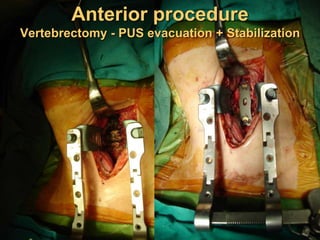
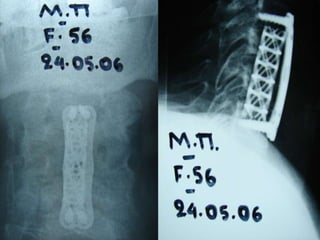
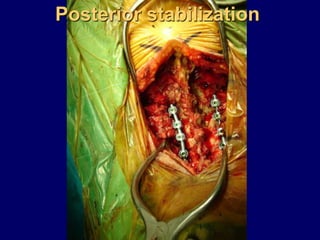


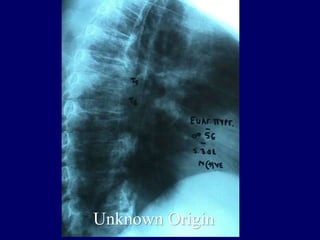



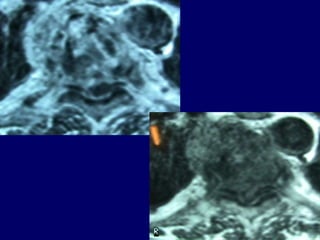
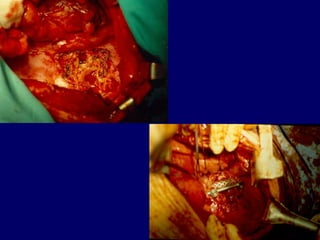
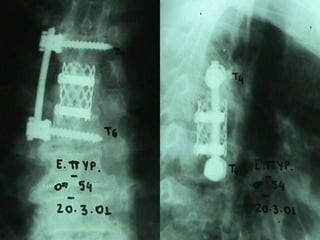







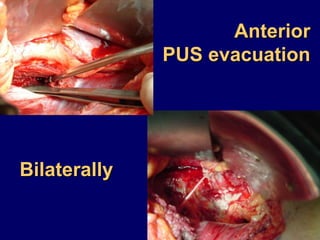

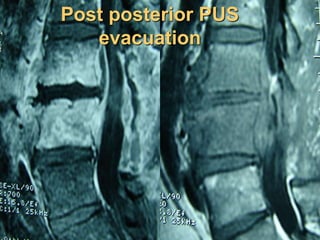
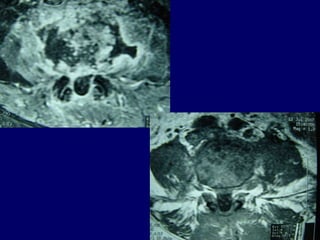
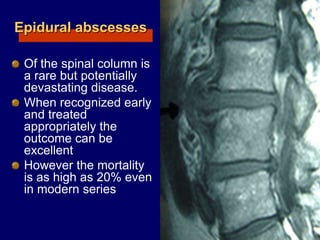

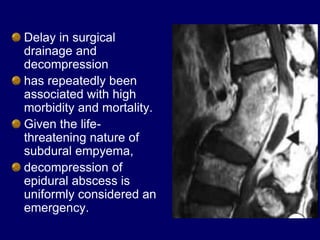

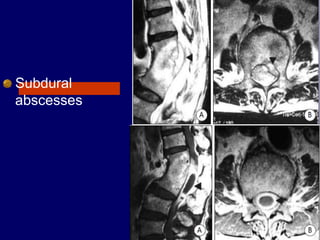

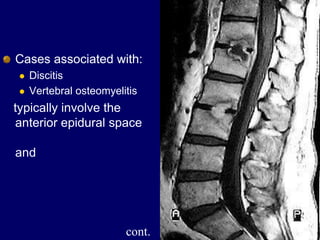



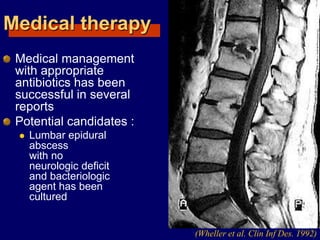

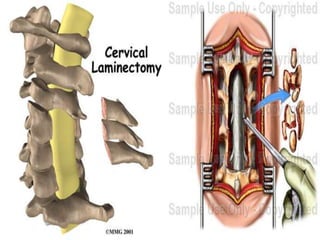
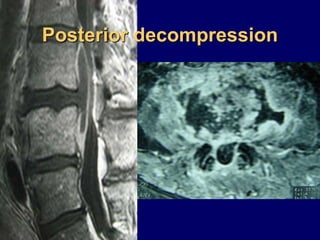




This document discusses four cases of vertebral osteomyelitis complicated by epidural abscesses. It describes the patients' symptoms, diagnostic findings including MRI and lab results, and treatments which involved surgical drainage and decompression followed by long-term IV and oral antibiotics. The author concludes that early surgical treatment along with antibiotics can allow for full neurologic recovery, but delays in surgery are associated with higher morbidity and mortality.























































![Espondilodiscite[1]](https://cdn.slidesharecdn.com/ss_thumbnails/espondilodiscite1-190205175546-thumbnail.jpg?width=640&height=640&fit=bounds)










































