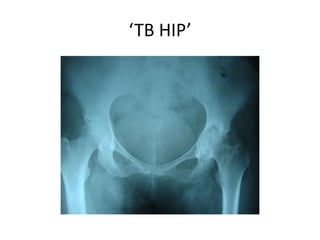
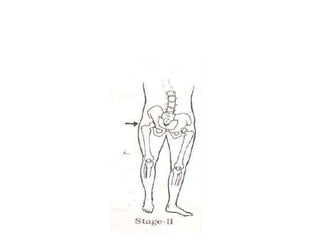
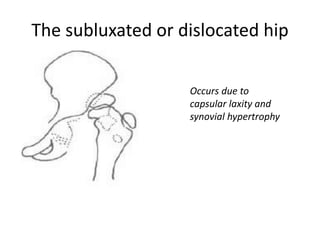
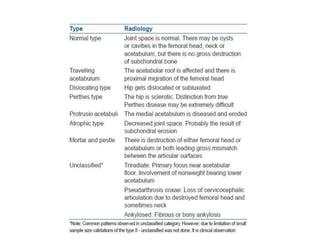
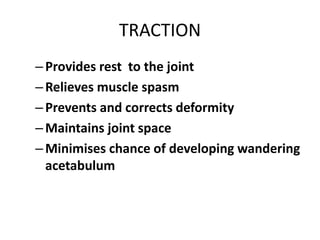
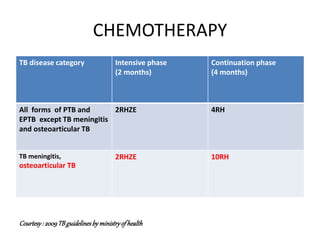
This document discusses tuberculosis of the hip joint. It begins by describing the causative organism, Mycobacterium tuberculosis, which is an acid-fast bacillus. It then covers the pathophysiology of tuberculosis infection in the hip, including the formation of tubercles and caseation necrosis. The document outlines the clinical presentation of TB of the hip and its radiographic appearance. It discusses the different stages of TB arthritis in the hip and associated radiographic findings. The document concludes by covering treatment approaches for TB of the hip including chemotherapy, traction, arthroplasty, arthrodesis and osteotomy.



![IMPORTANT OBSERVATIONS
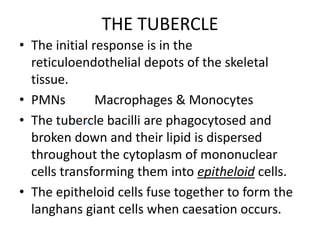
A] Childhood TB hip (growing period) chronic
hyperemia would lead to enlargement of
femoral head epiphysis and metaphysis
leading to COXA MAGNA.
B] Thromboembolic phenomena of selective
terminal vasculature create Perthe’s like
changes and reduced blood supply due to
effusion (tamponad effect) causing decrease
size of femoral head and neck – COXA BREVA.](https://image.slidesharecdn.com/40zifajkrou8dcjaheay-signature-ef734a3a2580a9c839befcba77ee24381806b98abf1b60a1fad9f3933be22eb9-poli-150731200513-lva1-app6892/85/Tuberculosis-of-the-hip-28-320.jpg)
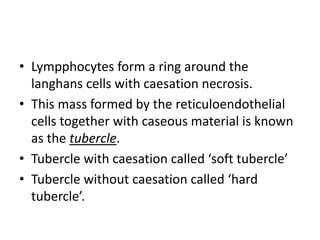
![C] Restricted growth of femoral capital epiphysis
with normal growth of trochanteric growth
plate lead to – COXA VARA.
D] Restricted growth of trochanteric physis with
normal growth of femoral epiphysis lead to -
COXA VALGA.](https://image.slidesharecdn.com/40zifajkrou8dcjaheay-signature-ef734a3a2580a9c839befcba77ee24381806b98abf1b60a1fad9f3933be22eb9-poli-150731200513-lva1-app6892/85/Tuberculosis-of-the-hip-29-320.jpg)
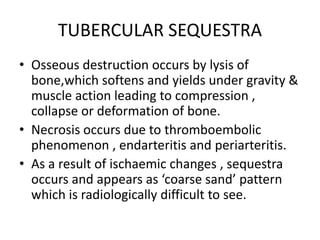
![E] A triad of radiologic abnormalities (Phemister
triad);
– periarticular osteoporosis
– peripherally located osseous erosion
– gradual diminution of joint space suggests the dx
of TB
F] Occasionally, wedge-shaped areas of necrosis
(kissing sequestra) in joint margin. These
marginal erosions may simulate RA](https://image.slidesharecdn.com/40zifajkrou8dcjaheay-signature-ef734a3a2580a9c839befcba77ee24381806b98abf1b60a1fad9f3933be22eb9-poli-150731200513-lva1-app6892/85/Tuberculosis-of-the-hip-30-320.jpg)























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


