Downloaded 1,289 times

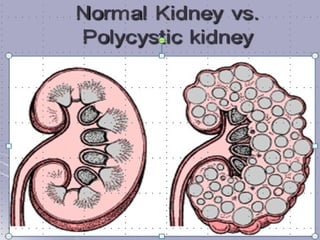
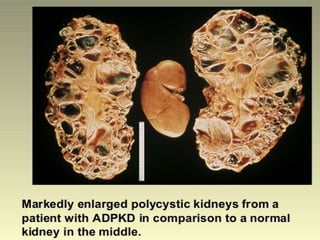
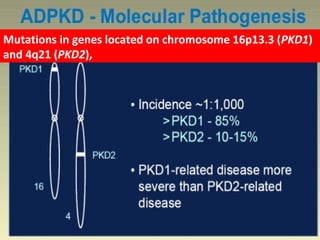
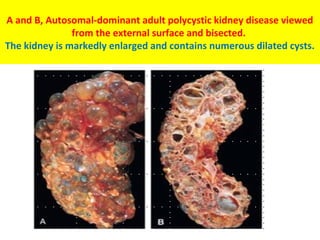
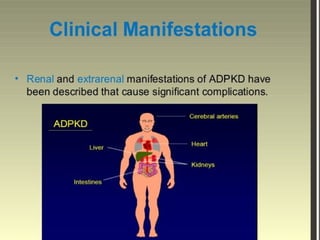
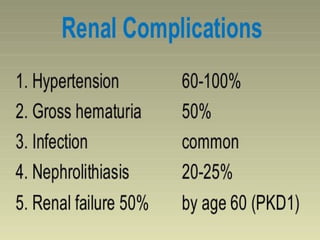
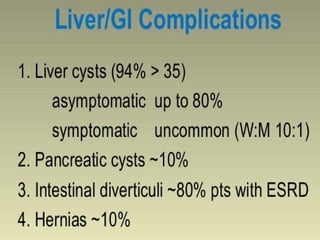
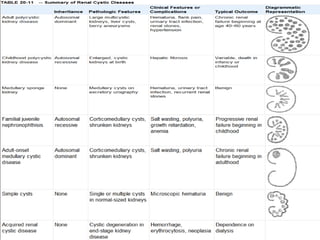


Polycystic kidney disease is caused by mutations in genes located on chromosomes 16p13.3 and 4q21. The kidneys become massively enlarged due to the growth of multiple cysts filled with fluid. Patients may be asymptomatic for years until renal insufficiency develops. Symptoms can include pain, bleeding, and high blood pressure as the cysts enlarge and damage the kidney tissue. Complications include liver and heart cysts as well as brain aneurysms. While the condition progresses slowly over decades, it ultimately leads to kidney failure and often death from heart or brain related issues.















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







