Downloaded 151 times

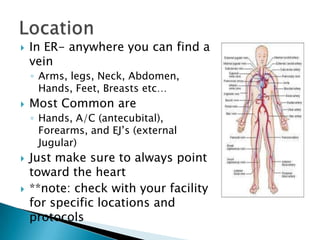
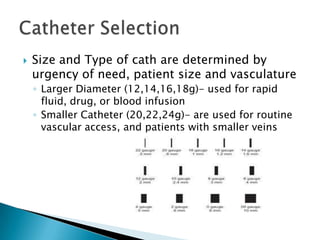
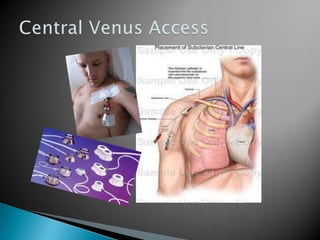


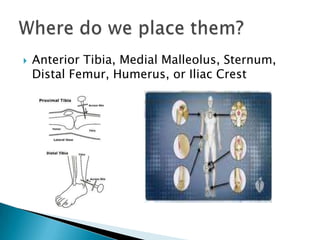


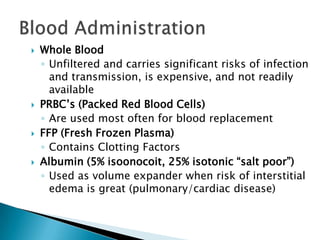
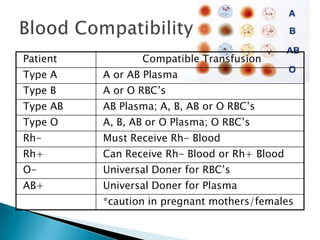
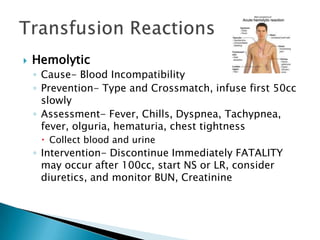

This document provides an overview of vascular access including peripheral access, central venous access, and intraosseous infusion. It discusses tips for obtaining peripheral access as well as potential complications. Common sites for peripheral access are noted. Factors such as urgency, patient size, and vasculature are discussed in selection of catheter size and type. Reasons for central line placement include unstable conditions, prolonged IV therapy, and long-term access needs. Intraosseous infusion is described as an alternative when other access is unavailable. Blood products and transfusion reactions are also summarized.
































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






