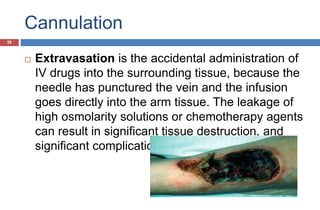
Intravenous (IV) therapy involves infusing liquids directly into veins. It has been used since the 1830s to treat cholera. Common uses of IV therapy include fluid replacement, medication delivery, blood transfusions, and total parenteral nutrition. IV fluids are categorized as crystalloids or colloids and can be isotonic, hypotonic, or hypertonic depending on their concentration of electrolytes. Various devices are used for IV access including needles, peripheral IV lines, central lines, and implanted ports. Precise control of infusion rates requires pumps. Potential risks include infection, phlebitis, infiltration of tissues, and embolisms.




![ Some patients may need bolus doses
of medications
In some instances, patients with
unstable physiologic status may have
an I.V. access site set up “just in case”
so that medications may be
administered rapidly if there is an
emergent or urgent indication
(e.g., amiodarone [Cordarone] and
epinephrine).](https://image.slidesharecdn.com/intravenous-140325040551-phpapp02/85/Intravenous-ther-21-320.jpg)