Downloaded 435 times









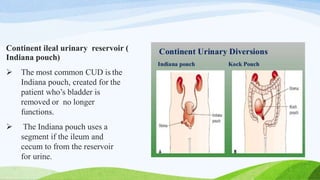

Urinary diversion procedures are performed to redirect urine flow from the bladder to a new exit site, often due to conditions like bladder cancer or pelvic malignancies. There are two main types: cutaneous urinary diversion, where urine drains through a stoma in the skin, and continent urinary diversion, which uses a segment of intestine to create a reservoir. Complications can arise from these complex procedures, necessitating careful post-operative monitoring and nursing management.























































































