Introduction
Urinary diversion, thererouting of urine flow
from the bladder, is indicated when the bladder is
removed (cystectomy) or non-functional due to
various conditions.
3.
Definition
• Urinary diversionis a surgical procedure to reroute
urine flow when the normal pathway is blocked or
damaged
4.
Specific indications forurinary
diversion:
• Bladder Cancer: The most frequent reason,
requiring cystectomy.
• Neurogenic Bladder: Conditions like spina bifida,
spinal cord injury, or multiple sclerosis can damage
the nerves controlling the bladder, leading to
dysfunction.
• Radiation Damage: Radiation therapy for pelvic
cancers can cause significant bladder damage,
necessitating diversion.
5.
• Severe Incontinence:When standard treatments
fail to manage urinary leakage.
• Trauma: Injuries to the bladder, urethra, or pelvis
can require diversion.
• Congenital Anomalies: Birth defects affecting
bladder development can be an indication
6.
• Chronic Inflammation:Conditions like interstitial
cystitis or recurrent infections can lead to severe
bladder damage.
• Tumors: Tumors in the genitourinary tract or
surrounding areas can also necessitate urinary
diversion.
• Urethral Obstruction: Conditions like enlarged
prostate or benign prostatic hyperplasia can cause
obstruction
7.
Types
• It canbe either continent, where the patient can
control urine drainage, or incontinent, where urine
constantly drains into an external bag
8.
• Continent diversionscreate a pouch within the
body, allowing for intermittent catheterization or
normal urination,
• while incontinent diversions involve a stoma
(opening) on the abdomen where urine is collected
in an external pouch.
9.
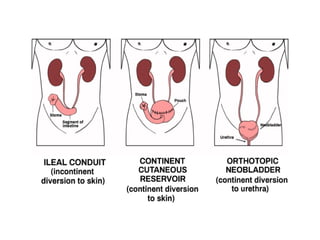
1. Incontinent UrinaryDiversion:
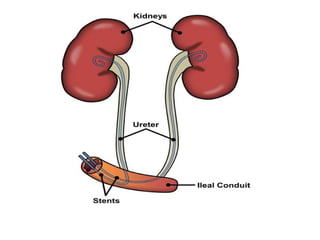
• leal Conduit:
This is the most common type. It involves
using a piece of the small intestine (ileum) to create a
passage (conduit) that is connected to the ureters
and brought out to the abdominal wall as a stoma.
Urine drains continuously into an external collection
pouch.
10.
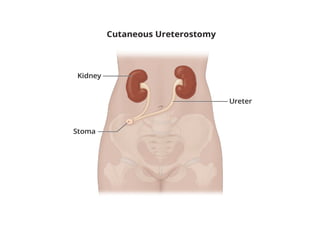
• Cutaneous Ureterostomy:
Aless common method where the ureters are
directly brought out to the abdominal wall as
separate stoma
11.
2. Continent UrinaryDiversion:
• Orthotopic Neobladder:
A pouch is created from a segment of the
intestine and connected to the urethra. The patient
can then urinate normally
12.
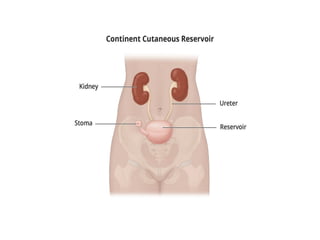
• Continent CutaneousReservoir (e.g., Indiana
Pouch):
A pouch is created from the intestine and
connected to a stoma on the abdominal wall.
Patients catheterize the stoma to drain the pouch.
13.
• Ureterosigmoidostomy:
The uretersare connected to the sigmoid colon,
allowing urine to drain with stool through the anus.
This method is rarely used due to high complication
rates.
14.
3. Other UrinaryDiversion Methods:
• Bladder Catheterization:
A catheter is inserted through the urethra into
the bladder to drain urine.
• Cystostomy:
A catheter is inserted directly into the bladder
through a small incision in the abdomen.
15.
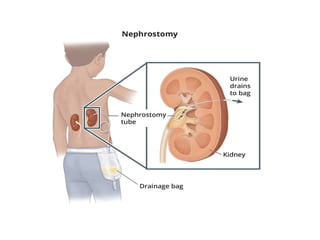
• Nephrostomy: Acatheter is inserted into the kidney
to drain urine.
• Ureteral Stent: A thin tube is placed in the ureter to
help drain urine from the kidney to the bladder or
from the ureter to an external drainage bag
21.
Early Complications:
• UrinaryLeakage: Can occur at the surgical site or
around the stoma (the opening in the abdomen for
urine drainage).
• Urinary Obstruction: Blockage of urine flow,
potentially due to swelling, scarring, or kinking of
the ureter.
• Fistula Formation: Abnormal connections between
the urinary tract and other organs or tissues.
22.
• Postoperative FluidCollection: Fluid buildup around
the surgical site, possibly requiring drainage.
• Infection: Urinary tract infections (UTIs) and
infections at the surgical site are common.
• Metabolic Acidosis: A buildup of acid in the body
due to the intestines' altered handling of
electrolytes and fluids.
• Electrolyte Imbalances: Disruptions in the body's
electrolyte balance, including low potassium,
calcium, or magnesium.
23.
Late Complications:
• StomalStenosis: Narrowing of the stoma, making it
difficult for urine to drain.
• Ureteroileal Anastomotic Stricture: Scarring and
narrowing at the connection between the ureter
and the ileal conduit (a common type of urinary
diversion).
• Urolithiasis: Formation of kidney stones or stones
within the urinary diversion.
• Parastomal Hernia: Protrusion of abdominal
contents through the abdominal wall around the
24.
• Ureteroarterial Fistula:Abnormal connection
between the ureter and an artery.
• Bowel Problems: Obstruction or diarrhea due to the
diverted urine affecting bowel function.
• Skin Problems: Irritation, infection, or breakdown of
the skin around the stoma.
25.
Management and Monitoring:
•Regular Monitoring: Patients with urinary diversion
require long-term monitoring for potential
complications.
• Imaging Studies: Radiological imaging, including CT
scans and ultrasounds, are used to assess the
urinary tract and detect abnormalities.
• Interventional Procedures: Minimally invasive
procedures, such as endoscopic stone removal or
stent placement, can be used to manage
complications
26.
• Medical Management:Treatment for metabolic
acidosis, electrolyte imbalances, and infections is
crucial.
• Surgical Correction: In some cases, surgical repair
or revision of the urinary diversion may be
necessary