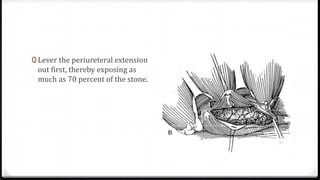
Downloaded 174 times


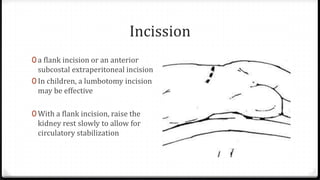
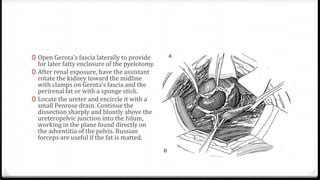
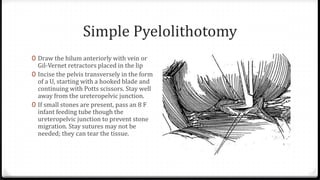

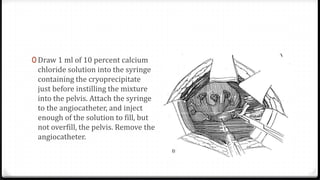
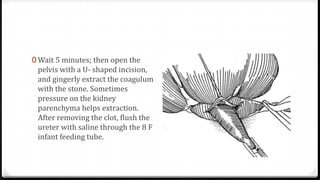
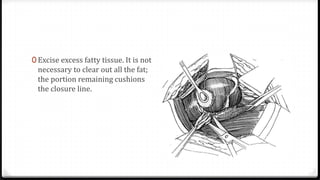
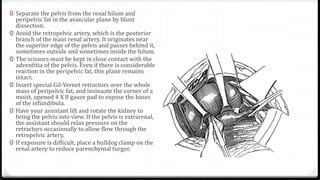
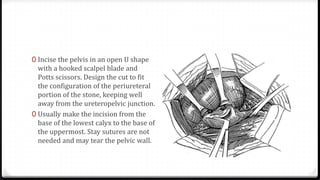
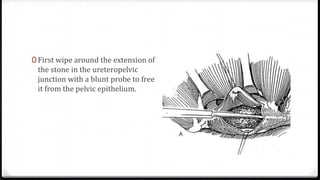
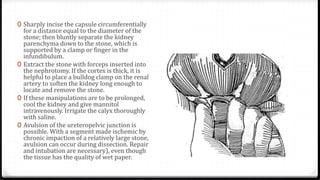

The document describes surgical procedures for removing kidney stones. It indicates that open surgery is still needed in cases of obstruction, infection, failed lithotripsy, or stones too large for other procedures. It then provides details on instruments, incisions, and techniques for simple pyelolithotomy, coagulum technique, extended pyelolithotomy, and managing stones extending into the ureteropelvic junction. The goal is to remove all stones and debris while minimizing damage to the kidney and ensuring the pelvis can be closed watertight.












































![Urolithiasis presented by Dr Muhammad nouman([Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/urolithiasisautosaved-1-250603143258-c924c676-thumbnail.jpg?width=640&height=640&fit=bounds)










































