Cryptorchidism
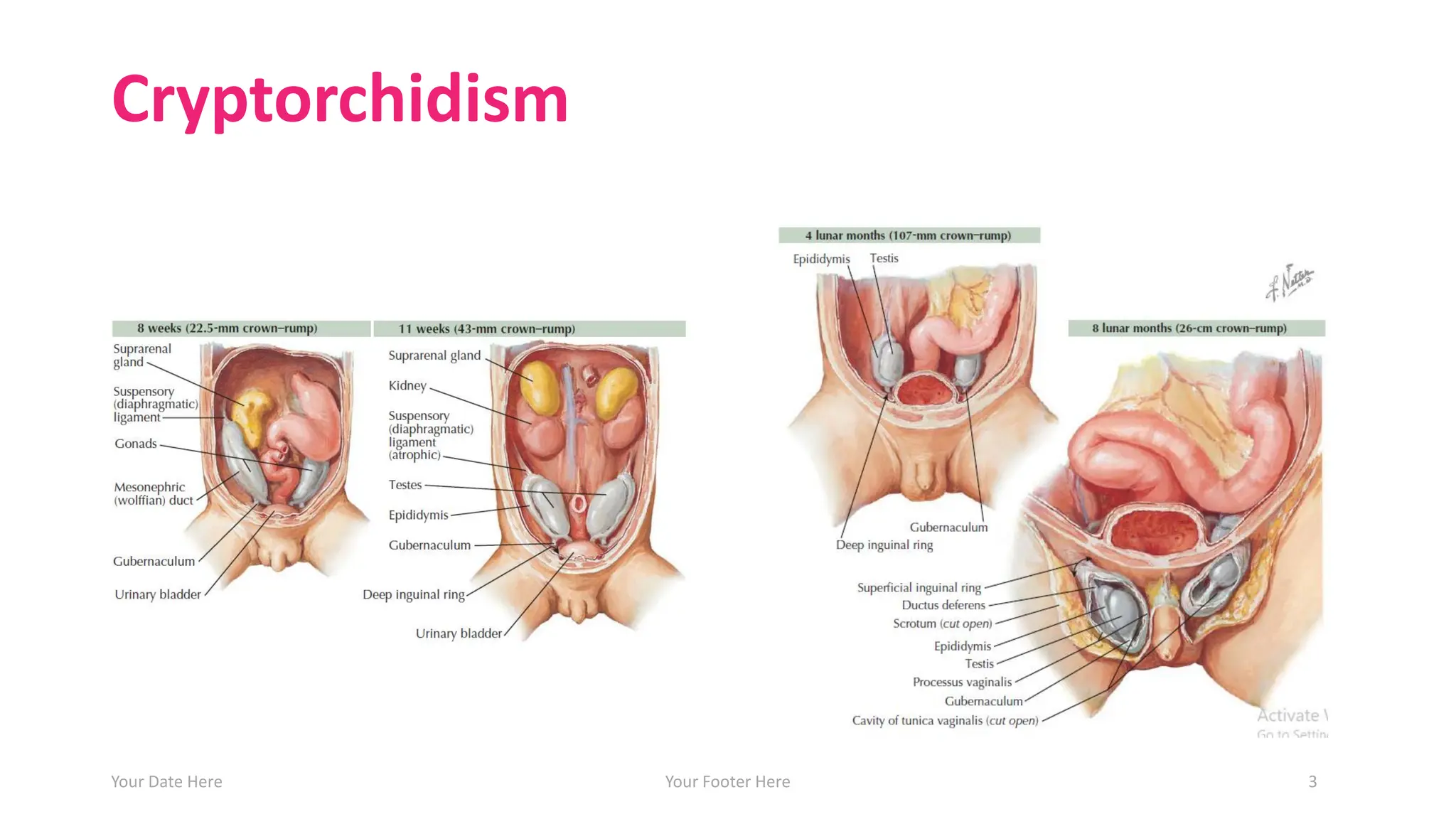
• Physiology oftesticular descent:
• 1st phase: from genital ridge→ internal inguinal ring (7-8
w), under influence of MIS acting on the gubernaculum
• 2nd phase: inguinal canal→ scrotum (24-28 w), under
influence of testosterone.
• Failure of descent→ congenital UDT (crypotorchidism).
• Definition:
• Failure of one or both testicles to descend to their
natural position in the scrotum
Your Date Here Your Footer Here 2
Cryptorchidism
• Incidence
• Incidenceis 3% at birth (unilateral > bilateral, Right > Left ).
• Approximately 80% will spontaneously descend by 3 months.
• The incidence at 3 months is 1% and at 1 year is 0.8%
• Risk factors
• Prematurity (incidence at <30wk gestation is 40%; most will
spontaneously descend if >2kg birthweight).
• LBW and SGA
• Twins and family history (father or brother, 4.6 or 6.9 times
relative risk, respectively).
Your Date Here Your Footer Here 4
Cryptorchidism
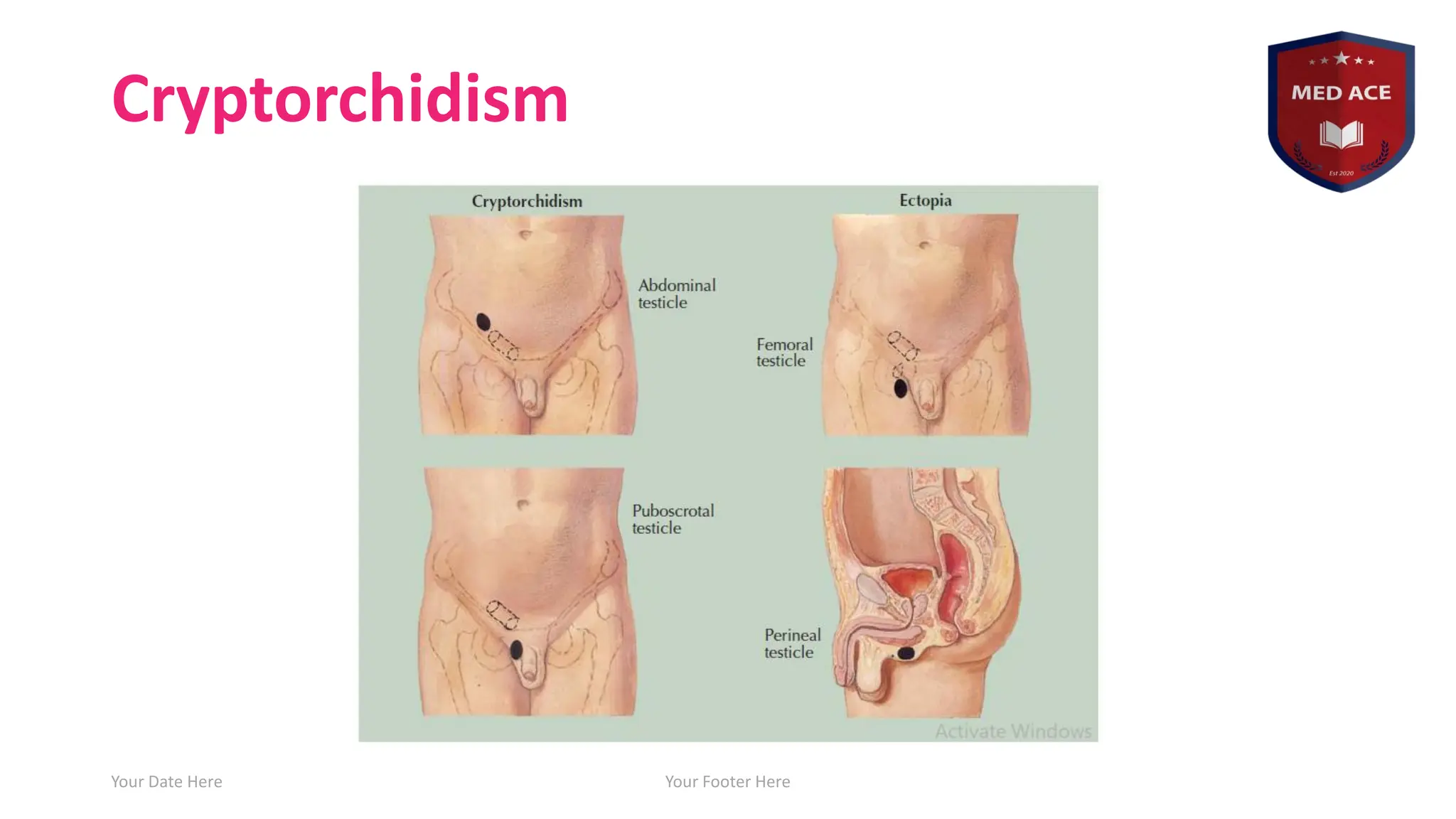
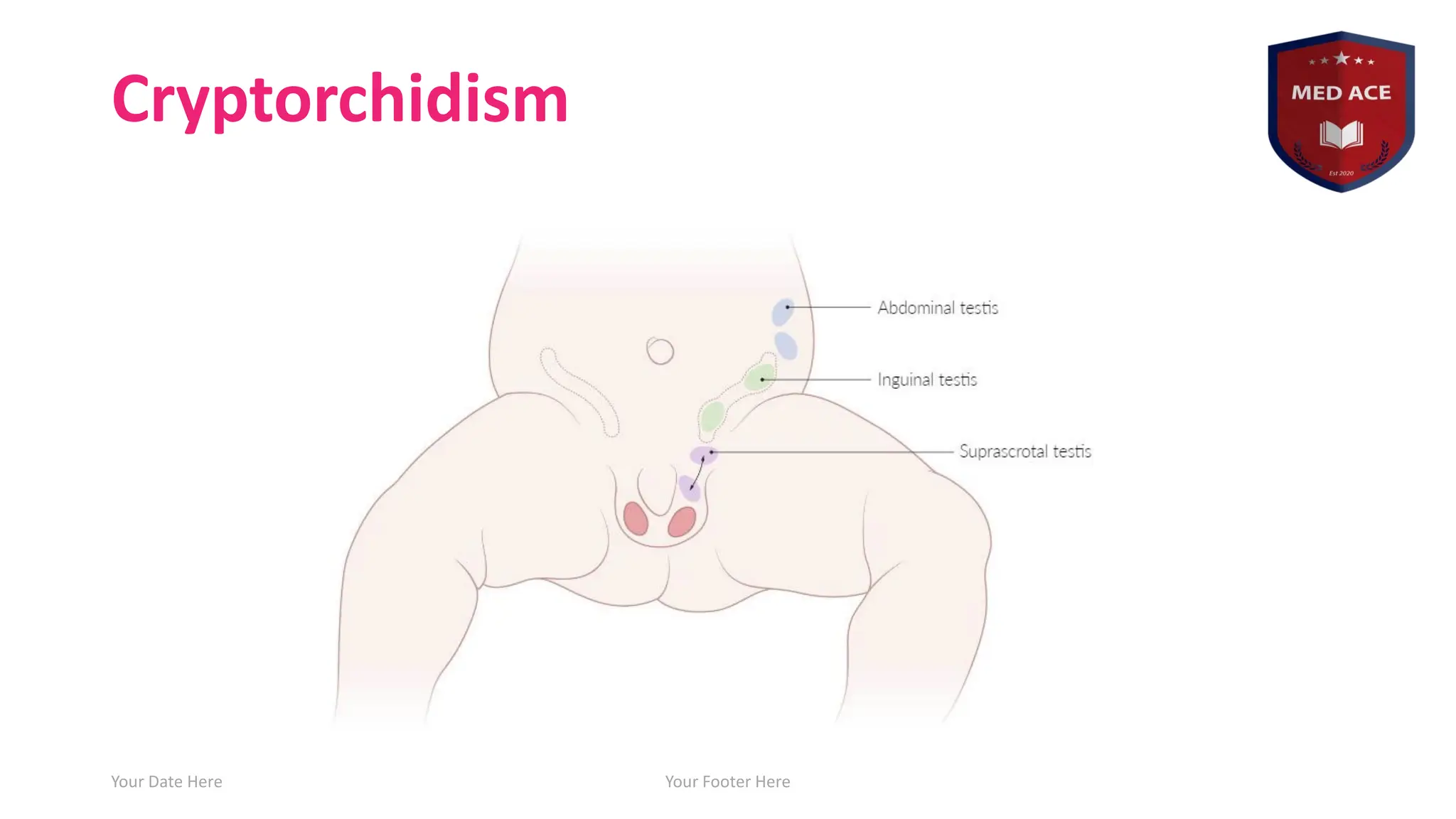
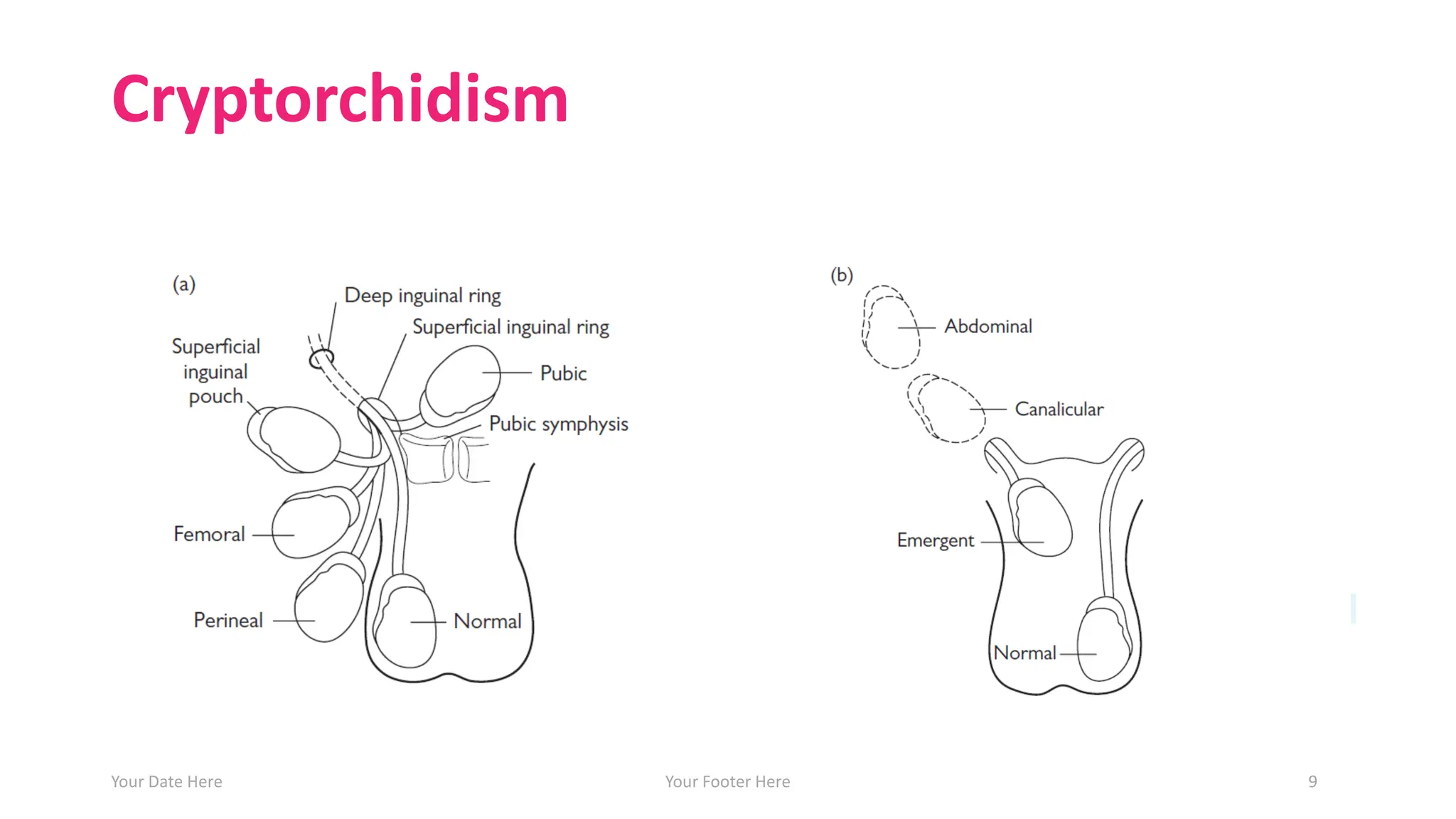
• Classification:
• 1.Incomplete descent (95%), testis not in the scrotum but
still present along its anatomical path of descent (intra-
abdominal, intra-inguinal, pre-scrotal).
• 2. Ectopic (<5%), abnormal testis migration below the
external ring of the inguinal canal (to the perineum, base of
the penis, or femoral areas)
• 3. Retractile (an intermittent active cremasteric reflex causes
the testis to retract up and out of the scrotum)
• 4. Atrophic/absent/vanishing.
• 5. Acquired UDT (testicular ascent).
Your Date Here Your Footer Here 6
Cryptorchidism
• Etiology
• Abnormaltestis or gubernaculum (tissue that guides the testis into the
scrotum during development);
• Endocrine abnormalities (low level of androgens, human chorionic
gonadotrophin [hCG], luteinizing hormone (LH), calcitonin gene–related
peptide)
• Decreased intraabdominal pressure (prune-belly syndrome,
gastroschisis).
• Pathology
• There is degeneration of Sertoli cells, loss of Leydig cells, and atrophy and
abnormal spermatogenesis.
• ♂ fertility depends on the transformation of gonocytes to adult dark
spermatogonia at 3– 6 months, and germ cell loss is preventable by
correcting the position of the testis.
Your Date Here Your Footer Here 10
11.
Cryptorchidism
• Complications
• Testicularcancer (germ cell tumors)
• 4-fold higher in unilateral undescended testis, 11-fold higher in bilateral. There
is a 4% lifelong risk of cancer with an intraabdominal Testis
• Most are seminomas; early orchidopexy slightly ↓risk of cancer
• There is a slightly increased risk of cancer in the contralateral, normally
descended testis.
• Infertility
• higher temperature of the abdominal cavity is suboptimal
for spermatogenesis → oligospermia → infertility.
• Paternity rate in unilateral UDT 80-90%, bilateral UDT 45-65%, orchidopexy can
↑fertility if performed <2 years.
• Testicular torsion (10 fold) or trauma
• Indirect Inguinal hernia due to patent processus vaginalis
Your Date Here Your Footer Here 11
12.
Cryptorchidism
• Clinical features
•Palpable (80% of cases)
• testicle cannot be manually manipulated into the scrotum
• intra-inguinal or pre-scrotal
• Impalpable (20% of cases)
• 40% intra-abdominal, 10% inguinal, 30% absent intra-
abdominal, and 20% absent intra-canalicular
Your Date Here Your Footer Here 12
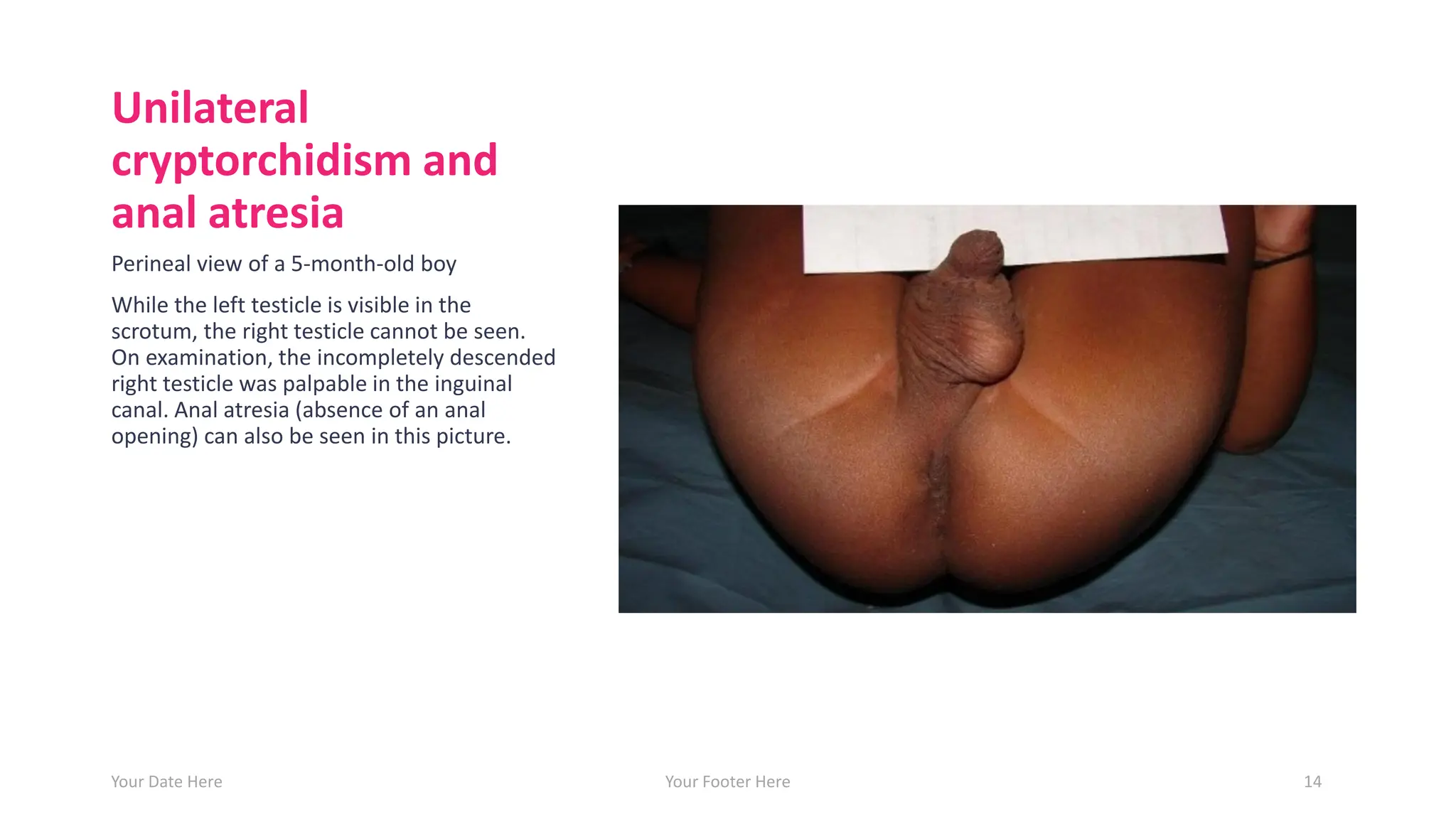
Unilateral
cryptorchidism and
anal atresia
Perinealview of a 5-month-old boy
While the left testicle is visible in the
scrotum, the right testicle cannot be seen.
On examination, the incompletely descended
right testicle was palpable in the inguinal
canal. Anal atresia (absence of an anal
opening) can also be seen in this picture.
Your Date Here Your Footer Here 14
15.
Cryptorchidism
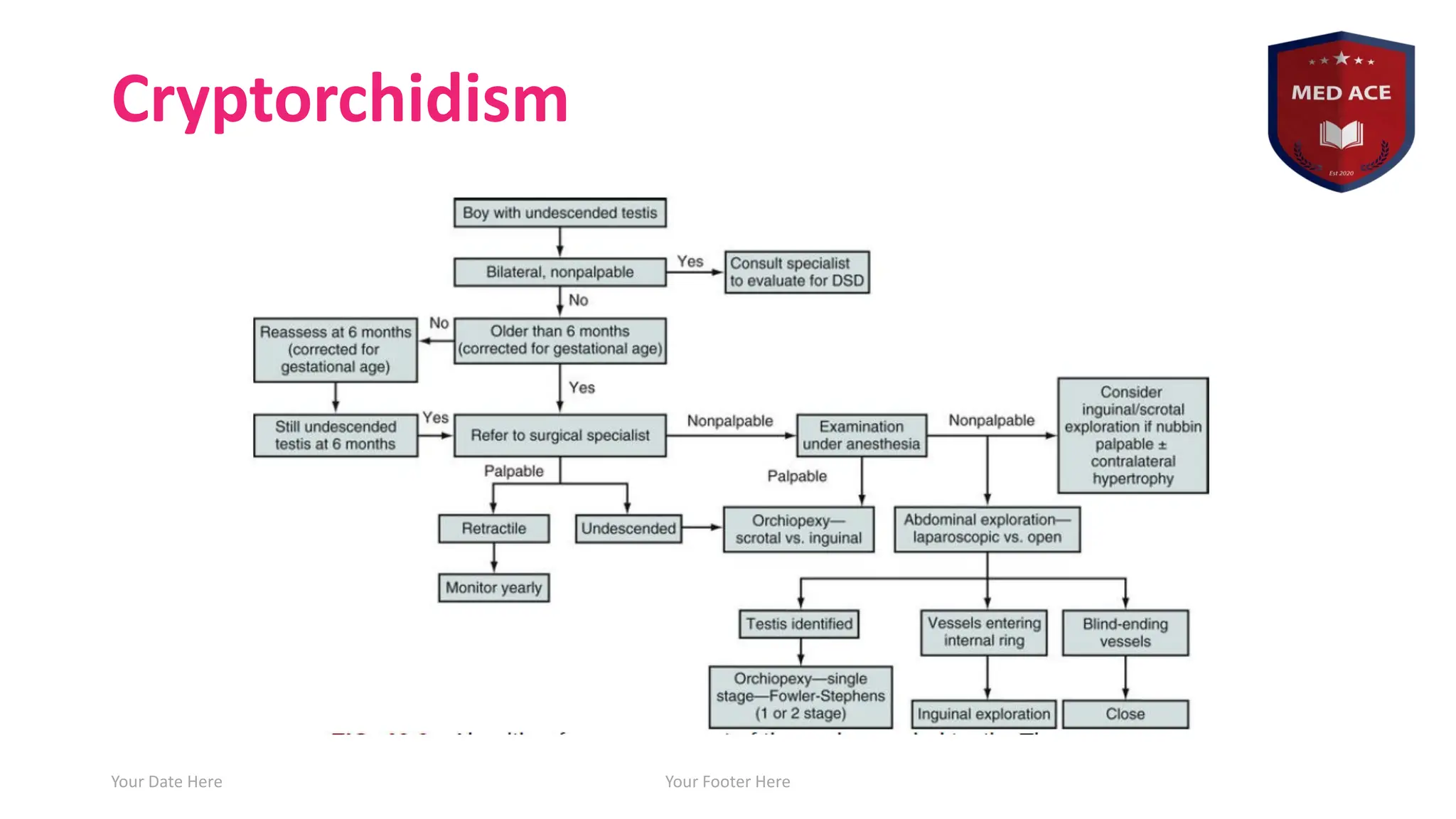
• Diagnosis
• Fullexamination is required (scrotum, inguinal canal)
• Palpable or not? If yes then where?
• Associated congenital defects (30% incidence if bilateral UDT)
• If neither testis is palpable, consider chromosome analysis (to
exclude an androgenized female) and hormone testing (high LH
and FSH with a low testosterone indicates anorchia)
• Inguino-scrotal US: can detect inguinal testis.
• Examination under anaesthesia (EUA) +/- laparoscopy (gold
standard to detect and treat intra-abdominal testis).
Your Date Here Your Footer Here 15
16.
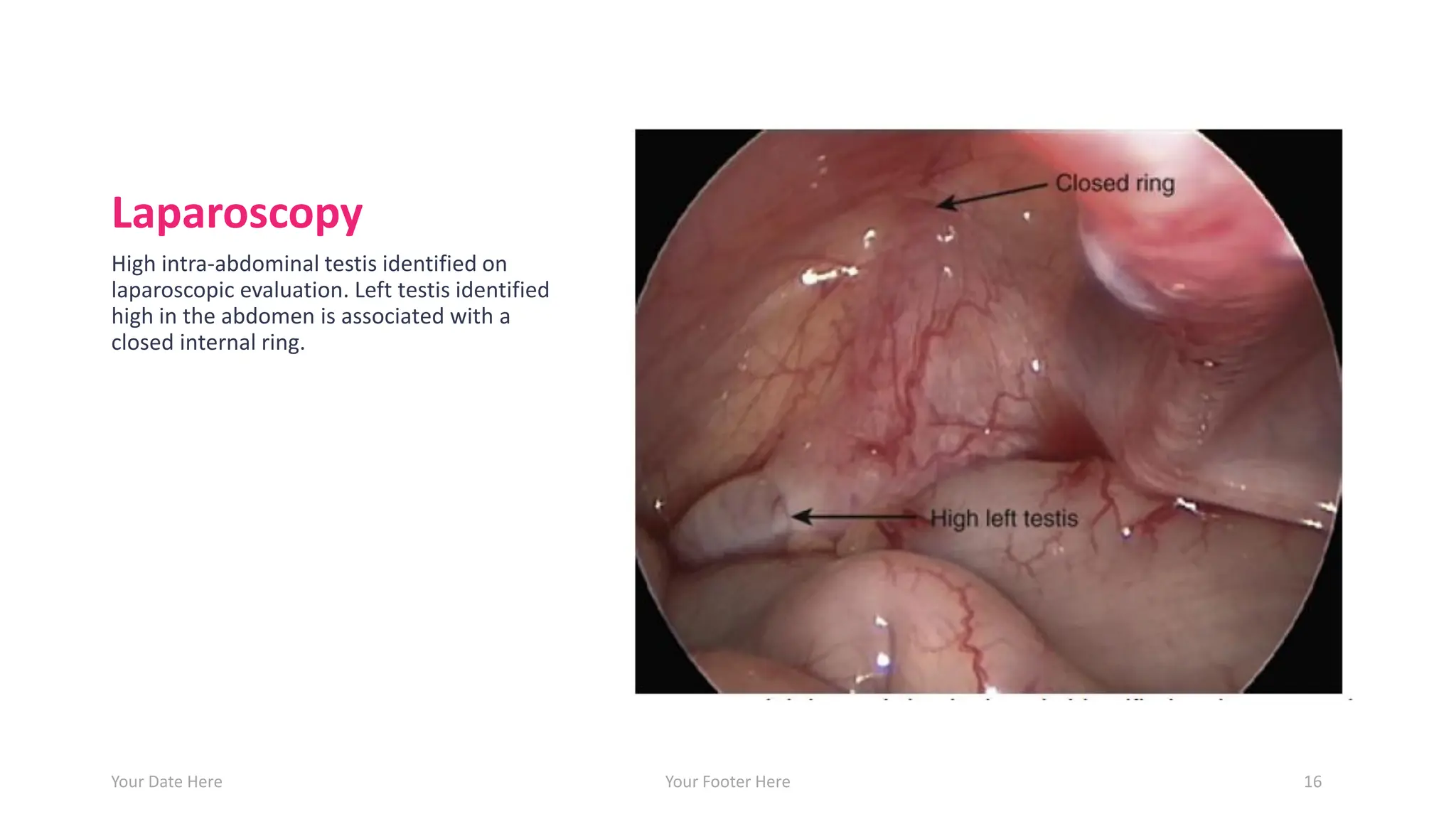
Laparoscopy
High intra-abdominal testisidentified on
laparoscopic evaluation. Left testis identified
high in the abdomen is associated with a
closed internal ring.
Your Date Here Your Footer Here 16
17.
Cryptorchidism
• Treatment
• Cryptorchidismtypically resolves without treatment via
spontaneous descent of testicles
• Persistent cases require surgery, which should be
performed as soon as possible between 3 and 12 months
• Orchiopexy (inguinal exploration, ligation of processus
vaginalis, bringing the testis into the scrotum and secure it
to sub-dartos pouch with sutures)
• Complications: testis atrophy, vas injury, re-ascent.
Your Date Here Your Footer Here 17
18.
Cryptorchidism
• Treatment
• Abdominal:
•Laparoscopic or open procedure (Fowler-Stephens):
• 1st stage: divide the spermatic vessels to provide extra length (testis
will rely on blood supply from vas).
• 2nd stage (after 6 months): bring testis to scrotum.
• Small, atrophic intra- abdominal testes (nubbin) require
orchidectomy ― orchidopexy of the contralateral normally
descended testis.
Your Date Here Your Footer Here 18
Other types
• Retractiletestis
• An intermittent active cremasteic reflex causes the testis to
migrate up and out of the scrotum.
• How to differentiate incomplete descent from retractile
testis:
• 1. Retractile can be brought back to scrotum without tension and it
will stay there for a while.
• 2. Retractile the affected hemi-scrotum is well-developed with
visible rugae.
• Treatment: Do regular follow-up. Most will descend
spontaneously and will not need orchidopexy.
Your Date Here Your Footer Here 20
21.
Other types
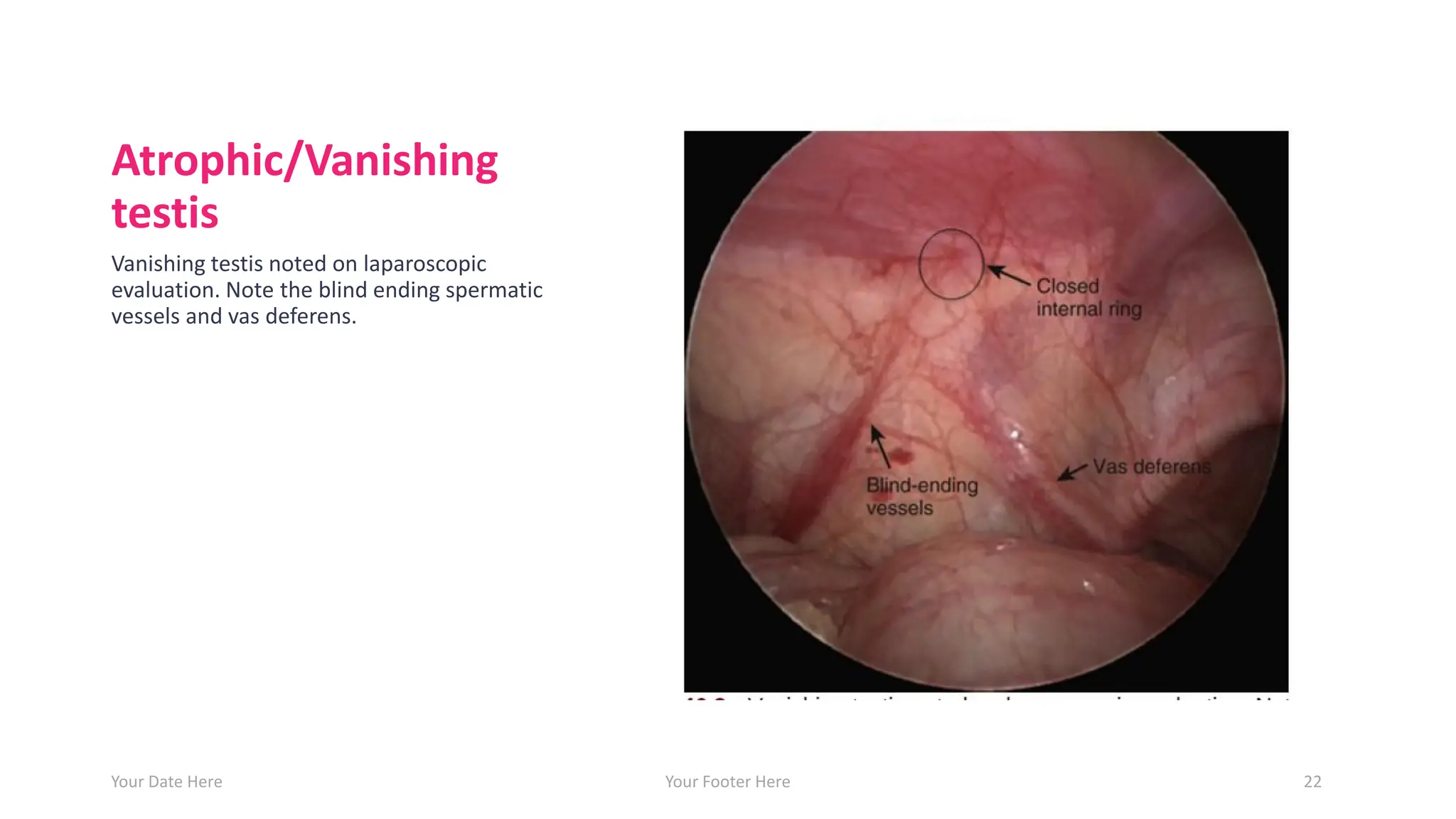
• Atrophic/Vanishingtestis
• Testis is atrophic/absent, usually due to in utero testicular
torsion, can be unilateral or bilateral.
• Unilateral:
• Associated with nubbin in ipsilateral scrotum.
• Associated with hypertrophy of the contralateral testis.
• Confirmed using laparoscopy by seeing blind-ending spermatic
vessels.
• Bilateral:
• Associated with micropenis.
• Associated with ↑FSH and LH levels, ↓ (testosterone, MIS, serum
inhibin B).
Your Date Here Your Footer Here 21
Other types
• Acquired(testicular ascent)
• Definition: a testis that was in the scrotum at birth but
ascended later in life (usually at an age of 7-9 years).
• Risk factors: retractile testis, patent processus vaginalis.
• Treatment: 20% will fail to descend into the scrotum at
puberty and thus required orchidopexy as the ‘ascended’
testis is at the same risk of degenerative changes as
congenital UDT.
Your Date Here Your Footer Here 23
![Cryptorchidism
• Etiology
• Abnormal testis or gubernaculum (tissue that guides the testis into the
scrotum during development);
• Endocrine abnormalities (low level of androgens, human chorionic
gonadotrophin [hCG], luteinizing hormone (LH), calcitonin gene–related
peptide)
• Decreased intraabdominal pressure (prune-belly syndrome,
gastroschisis).
• Pathology
• There is degeneration of Sertoli cells, loss of Leydig cells, and atrophy and
abnormal spermatogenesis.
• ♂ fertility depends on the transformation of gonocytes to adult dark
spermatogonia at 3– 6 months, and germ cell loss is preventable by
correcting the position of the testis.
Your Date Here Your Footer Here 10](https://image.slidesharecdn.com/cryptoorchidism-250818173840-2c6132b7/75/Cryptoorchidism-pdfjjdkdkkdkkkskksjddddr-10-2048.jpg)