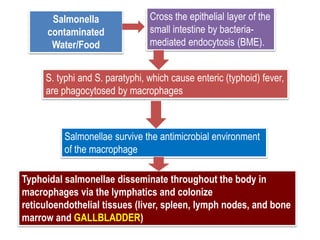
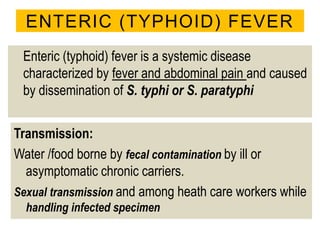
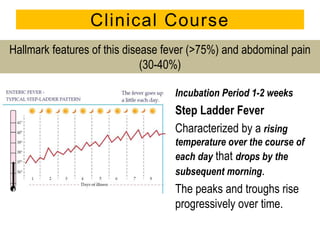
Ms. X, also known as Typhoid Mary, was an asymptomatic carrier of typhoid fever, with a history of spreading the disease across multiple households in the early 1900s. The document details the clinical features, transmission, diagnosis, and management of enteric (typhoid) fever caused by Salmonella typhi, including its symptoms, complications, and treatment options. Following her identification as a chronic carrier, Ms. X spent her life quarantined and died in 1938, with live typhoid bacteria found in her gallbladder upon autopsy.


















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

