
Recommended
More Related Content
What's hot
What's hot (20)
Similar to TTP.ppt
Similar to TTP.ppt (20)
More from AbdulKaderSouid
More from AbdulKaderSouid (12)
Recently uploaded
Recently uploaded (20)
TTP.ppt
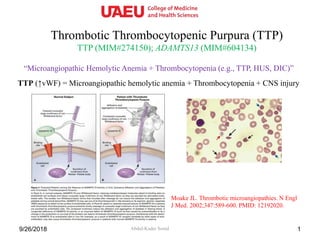
- 1. Thrombotic Thrombocytopenic Purpura (TTP) TTP (MIM#274150); ADAMTS13 (MIM#604134) Abdul-Kader Souid9/26/2018 1 “Microangiopathic Hemolytic Anemia + Thrombocytopenia (e.g., TTP, HUS, DIC)” TTP (↑vWF) = Microangiopathic hemolytic anemia + Thrombocytopenia + CNS injury Moake JL. Thrombotic microangiopathies. N Engl J Med. 2002;347:589-600. PMID: 12192020.
- 2. 9/26/2018 2
- 3. 9/26/2018 3
- 4. Patient • A 12-year-old boy has anemia and thrombocytopenia. – ↓Hemoglobin, ↑reticulocyte count, ↑RBC fragments (schistocytes), and hemoglobinuria → intravascular hemolysis. • His thrombocytopenia responded to plasma transfusion. • He then had recurrent seizures. 49/26/2018 Black arrows point to RBC fragments, red arrow points to a large platelet, and blue arrow to a spherocyte.
- 5. His CBC 59/26/2018 Anemia + thrombocytopenia + reticulocytosis
- 6. His Peripheral Blood Smear 69/26/2018 Microangiopathic hemolysis Arrows point to RBC fragments
- 7. His Urinalyses (UA) 79/26/2018 Hemoglobinuria Urine is free of RBC
- 8. von Willebrand factor-cleaving protease (VWFCP) deficiency → TTP • Autosomal recessive disease • Intravascular (microangiopathic) hemolysis • Consumptive thrombocytopenia • The pathologic process is reversed by plasma infusion • Seizure disorder 3) Factor VIII delivery 1) Platelet adhesion to collagen 2) Platelet-platelet spreading and aggregation Collagen vWF GPIb- Platelet GPIIb/IIIa vWF Fibrinogen Platelet Factor VIII -S-S- -S-S- Results of his work-up: • von Willebrand factor-cleaving protease (VWFCP) activity <5% (normal, ≥67%) • VWF antigen and activity are normal. • VWF Multimer Analysis = ↑molecular weight multimers
- 9. • Von Willebrand factor (VWF) is a multimeric plasma glycoprotein that mediates platelet adhesion and aggregation. • ADAMTS13 is a protease that cleaves VWF in circulating blood and thereby limits platelet aggregation. Familial Thrombotic Thrombocytopenic Purpura = von Willebrand Factor-Cleaving Protease Deficiency = ADAMTS13 Deficiency • His ADAMTS13 gene sequencing shows homozygous splice site mutation, c.2234+2T>C in ADAMTS13. • ADAMTS13: “A Disintegrin-like and metalloproteinase with thrombospondin type 1 motif, member 13”. • ADAMTS13 gene is located at: 9q34.2. MIM#604134 (http://omim.org/entry/604134)
- 10. • In patients with TTP, abnormally large VWF multimers in the plasma cause excessive intravascular platelet aggregation. • These extremely adhesive VWF multimers arise due to a deficiency of VWF-cleaving protease. 109/26/2018 Blood 1997;89:3097-3103 Familial Thrombotic Thrombocytopenic Purpura = von Willebrand Factor-Cleaving Protease (VWFCP) Deficiency = ADAMTS13 Deficiency
- 11. • All studied six patients with familial TTP lacked vWF–cleaving protease activity, but had no inhibitor. • Of studied 24 patients with non-familial TTP, an inhibitor (IgG) of vWF– cleaving protease was found in 20 of these patients. • All 10 patients with familial HUS had normal protease activity. • All 13 patients with non-familial HUS had normal or slightly protease activity. 119/26/2018 NEJM 1998;339:1578-1584 Familial Thrombotic Thrombocytopenic Purpura = von Willebrand Factor-Cleaving Protease (VWFCP) Deficiency = ADAMTS13 Deficiency
- 12. • Mutations in a member of the ADAMTS gene family cause thrombotic thrombocytopenic purpura. • Proteolysis of VWF observed in normal plasma is decreased in TTP patients. • In four pedigrees of humans with congenital TTP, the responsible protease was mapped to chromosome 9q34. • A predicted gene in the identified interval corresponded to a new member of the ADAMTS family of zinc metalloproteinase genes (ADAMTS13). • Analysis of patients' genomic DNA identified 12 mutations in the ADAMTS13 gene, accounting for 14 of the 15 disease alleles studied. • Deficiency of ADAMTS13 is the molecular mechanism responsible for TTP. • Physiologic proteolysis of VWF and other ADAMTS13 substrates is required for normal vascular homeostasis. 129/26/2018 Familial Thrombotic Thrombocytopenic Purpura = von Willebrand Factor-Cleaving Protease (VWFCP) Deficiency = ADAMTS13 Deficiency Nature 2001;413:488-94.
- 13. Familial Thrombotic Thrombocytopenic Purpura von Willebrand Factor-Cleaving Protease (VWFCP) Deficiency ADAMTS13 Deficiency 9/26/2018 13 Day Treatment Hemoglobin (g/L) Platelet count (x109/L) Hemoglobinuri a ADAMTS13 activity -1 - 100 99 Small <5% 0 Plasma 10.9 118 Small 19 1 - 10.3 103 Small 31 6 - 11.8 203 Negative 12 8 - 11.9 264 Negative 18 10 - 11.8 188 Negative <10 17 - 11.6 114 Trace <10 20 - 11.0 33 Large <10 22 Plasma 10.7 22 Moderate 23 Plasma infusion every two weeks is recommended as the treatment of choice.
- 14. A 17-year-old girl presents with pallor, bruising and seizure. Her examination shows significant pallor and purpura. Her lymph nodes, liver, and spleen are normal. Her WBC count is 8 x109/L (normal, 5 to 10), hemoglobin concentration 73 g/L (normal, 110 to 130), reticulocyte count 318 x109/L (normal, 35 to 100), and platelet count 65 x109/L (normal, 150 to 400). Blood smear shows numerous schistocytes with a markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. Her serum creatinine is normal. Her urinalysis is remarkable for 2 RBC per high power field (normal, <5) and 3+ hemoglobin (normal, negative). She received plasma infusion, which promptly improved her thrombocytopenia. Which one of the following results on further investigation is correct? A. Complement dysregulation (hemolytic uremic syndrome) B. Mutation in ADAMTS13 gene (thrombotic thrombocytopenic purpura) C. Low von Willebrand factor (VWD) D. Positive direct antiglobulin test for IgG (autoimmune hemolytic anemia) E. Missing CD59 on the surface of blood cells (paroxysmal nocturnal hemoglobinuria) 14
- 15. Which one of the following diagnoses is correct? A. Macrophage activation syndrome (MAS) B. Hemolytic uremic syndrome (HUS) C. Thrombotic thrombocytopenic purpura (TTP) D. Hemophagocytic lymphohistocytosis (HLH) E. Disseminated intravascular coagulopathy (DIC) 15 A 17-year-old girl presents with pallor, bruising and seizure. Her examination shows significant pallor and purpura. Her lymph nodes, liver, and spleen are normal. Her WBC count is 8 x109/L (normal, 5 to 10), hemoglobin concentration 73 g/L (normal, 110 to 130), reticulocyte count 318 x109/L (normal, 35 to 100), and platelet count 65 x109/L (normal, 150 to 400). Blood smear shows numerous schistocytes with a markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. Her serum creatinine is normal. Her urinalysis is remarkable for 2 RBC per high power field (normal, <5) and 3+ hemoglobin (normal, negative). She received a fresh frozen plasma infusion, which promptly improved her thrombocytopenia.
- 16. Which one of the following treatments is correct? A. Eculizumab (for HUS and PNH) B. Packed red cell transfusion (for AHA) C. Platelet transfusion (for bone marrow failure syndromes) D. Plasma exchange (for TTP and HUS) E. Immunoglobulin transfusion (for ITP) 16 A 17-year-old girl presents with pallor, bruising and seizure. Her examination shows significant pallor and purpura. Her lymph nodes, liver, and spleen are normal. Her WBC count is 8 x109/L (normal, 5 to 10), hemoglobin concentration 73 g/L (normal, 110 to 130), reticulocyte count 318 x109/L (normal, 35 to 100), and platelet count 65 x109/L (normal, 150 to 400). Blood smear shows numerous schistocytes with a markedly reduced number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. Her serum creatinine is normal. Her urinalysis is remarkable for 2 RBC per high power field (normal, <5) and 3+ hemoglobin (normal, negative). She received plasma infusion, which promptly improved her thrombocytopenia.
- 17. Which one of the following managements is correct? A. Stool studies for Escherichia coli serotype O157:H7 B. Monitor hemoglobin concentration, platelet count, and serum creatinine C. Platelet transfusion D. Packed red blood cell transfusion E. Plasma exchange 17 A 17-year-old girl presents to the emergency department with pallor, fatigue and abnormal bruises. Her examination shows significant pallor, mild jaundice, and ecchymosis mostly in her extremities. Her lymph nodes, liver, and spleen are normal. Her WBC count is 8 x109/L (normal, 5 to 10), hemoglobin concentration 73 g/L (normal, 110 to 130), reticulocyte count 318 x109/L (normal, 35 to 100), and platelet count 65 x109/L (normal, 150 to 400). Blood smear shows schistocytes with decreased number of platelets. PT/INR, aPTT, TT, fibrinogen, and D-Dimer level are normal. Her serum creatinine is normal. Her urinalysis is remarkable for 2 RBC per high power field (normal, <5) and 3+ hemoglobin (normal, negative).
- 18. Required Reading • George JN. Clinical practice. Thrombotic thrombocytopenic purpura. N Engl J Med 2006;354:1927. • George JN. How I treat patients with thrombotic thrombocytopenic purpura: 2010. Blood 2010;116:4060. • Levy GG, Nichols WC, Lian EC, et al. Mutations in a member of the ADAMTS gene family cause thrombotic thrombocytopenic purpura. Nature 2001;413:488. 9/26/2018 18
- 19. 9/26/2018 19