
More Related Content
What's hot
What's hot (20)
Similar to Hemophilia.ppt
Similar to Hemophilia.ppt (20)
More from AbdulKaderSouid
More from AbdulKaderSouid (14)
Recently uploaded
Recently uploaded (20)
Hemophilia.ppt
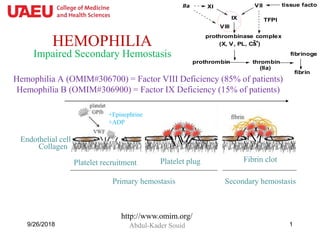
- 1. HEMOPHILIA Abdul-Kader Souid9/26/2018 1 Hemophilia A (OMIM#306700) = Factor VIII Deficiency (85% of patients) Hemophilia B (OMIM#306900) = Factor IX Deficiency (15% of patients) http://www.omim.org/ Collagen Endothelial cell Platelet recruitment Platelet plug Fibrin clot Primary hemostasis Secondary hemostasis +ADP +Epinephrine Impaired Secondary Hemostasis prothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII IIa TFPI
- 2. 9/26/2018 2
- 4. • Patients are males (affecting 1 per 5,000 males) - Females are carriers (X-linked recessive). • Symptoms usually begin by one year of age, at the time of crawling and walking. • The hallmark of hemophilia is bleeding into joints (hemarthrosis) and muscles (hematoma). • Intracranial bleeding is the leading cause of death. 9/26/2018 4 Factor VIII Deficiency female male
- 5. 1. Positive maternal history exists in 2/3 of patients; 1/3 have de novo mutations. 2. Clinical bleeding (joint, muscle, post-op) 3. ↑aPTT that corrects when mixing equal volume of normal plasma with patient plasma (i.e., factor deficiency). PT/INR, TT, platelet count, and vWF are normal. 4. Factor VIII activity is <30 units/dL (normal, 50-150 units/dL): – Severe disease (Factor VIII activity <1 unit/dL) occurs in 50% of patients (spontaneous bleeding, 90% develop joint disease) – Moderate disease (Factor VIII activity 1-5 unit/dL); bleeding occurs after trauma or surgery – Mild disease (Factor VIII activity >5 unit/dL) Factor VIII Deficiency: Diagnosis 9/26/2018 5 Must know
- 6. • Initial symptoms are warmness and tingling sensation, which require immediate replacement. • As blood fills the joint space, swelling, pain and limitation of movements occur (late symptoms). • Bleeding into a target joint (a joint that patient bleeds into repetitively) produces progressive synovitis and irreversible arthropathy. Knee MRI with a bleeding inside the joint Factor VIII Deficiency: Hemarthrosis JOINT BLEEDING SHOULD BE TREATED AT THE EARLIEST SYMPTOMS TO AVOID IRREVERSIBLE DAMAGES. THE JOINT SHOULD BE KEPT AT REST, BY USING CRUTCHES FOR WEIGHT BEARING JOINTS OR SLING/SPLINTING FOR JOINT SUPPORT. LIMB ELEVATION, ICE PACKING AND WRAPPING ARE RECOMMENDED. 6 Must know
- 7. Joint Disease in Hemophilia • Joint disease occurs in 90% of patients with severe hemophilia. – The frequency of joint bleeding is 15 ± 12 per year. – At least 50% of patients have restricted activity. • Prophylaxis treatment prevents joint bleeding and damage and is cost-effective; this modality should be the goal of therapy to preserve the joints. – Prophylaxis starts before 3 years of age and before any joint damage. Keep trough factor level ≥2%. – 15 to 40 units/kg rFVIII (or rFIX) every 2 to 3 days. 9/26/2018 7 Must know
- 8. • Hemophilia A is treated by recombinant factor VIII infusion (produced by cell lines transfected with human factor VIII gene; thus, avoiding the infectious risk of plasma-derived transfusion-transmitted diseases). • One unit/kg ↑plasma level by two units/dL; half-life = 8 h. • For mild-to-moderate bleeding (joint, laceration, minor trauma) give 25 units/kg (↑plasma level to 50 units/dL). • For moderate-to-severe bleeding (surgery, major trauma, intracranial, retroperitoneal, pharyngeal or neck bleeding) give 50 units/kg (↑plasma level to 100 units/dL) + monitor factor VIII level. Factor VIII On-Demand Replacements • Calculate the rFactor VIII dose for a 20-kg patient with a mild joint bleeding. Dose = 25 units/kg x 20 kg = 500 units (↑plasma level to 50 units/dL). 9/26/2018 8 Must know • Calculate the initial rFactor VIII dose for a 20-kg patient with a major trauma. Dose = 50 units/kg x 20 kg = 1,000 units (↑plasma level to 100 units/dL).
- 9. (1) Aminocaproic acid (Amicar; DrugBank name DB04134), not available in the UAE. 9/26/2018 9 Fibrinolytic inhibitors for Mucosal Bleeding (2) Tranexamic Acid (DB00302); available in the UAE. Must know (halt fibrinolysis by inhibiting plasminogen & plasmin) http://www.drugbank.ca/ The antifibrinolytic drugs are indicated for mucosal bleeding due to factor VIII, factor IX, or vWF deficiency. The World Federation of Hemophilia guidelines recommend oral tranexamic acid (1 g/dose or 10 mg/kg per dose 3 times daily) or aminocaproic acid (50 mg/kg 4 times daily with a maximum dose of 24 g daily) the day before dental surgery and then for a total of 7 days. “Fibrin glue” (fibrinogen + thrombin) is also used for local hemostasis during dental procedures.
- 10. • Desmopressin acetate (1-deamino-8-d-arginine vasopressin, or DDAVP) is the treatment of choice for mild-to-moderate factor VIII deficiency with minor bleeding. • It ↑factor VIII (and von Willebrand factor) level by 3-5 fold within 30 to 60 min of administration. • IV desmopressin (DDAVP Injection) is given at 0.3 g/kg in 50 mL of 0.9% NaCl over 30 min. • Intranasal desmopressin [Stimate Nasal Spray, one (150 g) or two (300 g) puffs] is equally effective. Desmopressin: Only for Factor VIII or VWF Deficiency Vasopressin Phe Gln NH2-Cys-S-S-Cys-Pro-L-Arg-Gly-NH2 Tyr Asn AsnTyr Cys-S-S-Cys-Pro-D-Arg-Gly-NH2 GlnPhe DDAVP [1-(deamino)-8-D-arginine vasopressin 9/26/2018 10 Must know Desmopressin is only indicated for mucosal bleeding due to factor VIII or VWF deficiency.
- 11. • This X-linked recessive disorder affects 1 in ~50,000 males. – About 1/3 of patients have a de novo mutation. • The clinical presentation is indistinguishable from hemophilia A. Factor IX Deficiency • Treatment is recombinant factor IX. • One unit/kg ↑plasma level by one unit/dL; half-life is ~24 h. – For mild-to-moderate bleeding (e.g., joint, muscle, laceration) give 50 units/kg (↑plasma level to 50 units/dL). – For moderate-to-severe bleeding (e.g., surgery, major trauma, intracranial, retroperitoneal, pharyngeal, neck) give 100 units/kg (↑plasma level to 100 units/dL). – Tranexamic Acid is also given for oral or dental bleed. – Desmopressin is ineffective in hemophilia B. • The rFactor IX dose for a 20-kg patient who has a joint bleeding is 50 units/kg x 20 kg = 1,000 units (↑plasma level to 50 units/dL). 11 Must know
- 12. Treatment of hemophilia Deficiency Treatment Dosing Factor VIII Recombinant factor VIII Mild-to-moderate bleeding: 20-30 units/kg.1 Moderate-to-severe bleeding: 40-75 units/kg.1 Desmopressin DDAVP Injection: 0.3 µg/kg iv or sc. (single daily dose).2 Stimate Nasal Spray: One or two sprays (single daily dose).2 Antifibrinolytic drugs Aminocaproic acid: 50 mg/kg every 6-8 h (max. 24 g daily) x 7 days. OR Tranexamic acid: One g/dose or 10 mg/kg/dose 3 times daily x 7 days. Factor IX Recombinant factor IX Mild-to-moderate bleeding: 50-70 units/kg.3 Moderate-to-severe bleeding: 100-120 units/kg.3 Antifibrinolytic drugs As above 1, For repetitive infusions, factor VIII is commonly given every 8-12 h; 2, the same dose can be repeated once a day for 3-5 days if necessary; 3, For repetitive infusions, factor IX is commonly given every 12-24 h.
- 13. Required Reading • Manco-Johnson MJ, Abshire TC, Shapiro AD, et al., Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357:535-44. • den Uijl I, Biesma D, Grobbee D, Fischer K. Turning severe into moderate haemophilia by prophylaxis: are we reaching our goal? Blood Transfus. 2013;11:364-9. • http://www1.wfh.org/publications/files/pdf-1472.pdf • Handout in the Blackboard. 9/26/2018 13
- 14. • The disease is X-linked recessive (heterozygous females are asymptomatic). • About ½ of male patients with severe disease have intron 22 inversion, which shuts down the gene expression. Factor VIII Deficiency 9/26/2018 14 Optional
- 15. • Ileopsoas bleeding (may follow heavy lifting or strenuous exercise) causes leg flexion, pain in the anterior surface of the thigh (femoral nerve compression) and inability to extend the leg. • Abdominal bleeding (into the liver, spleen, pancreas or retroperitoneum) produces falling hemoglobin and abdominal pain. • Buttock, thigh and forearm bleeding may produce neurovascular compression (compartment syndrome). • Neck or oral hematoma cause dyspnea, dysphagia and compromise airway. Factor VIII Deficiency: Hematoma • Psoas bleeding causes pain in the right lower quadrant, resembling appendicitis or hip problem. These situations require immediate replacement and close observation. 9/26/2018 15 Optional
- 16. • Arterial sticks and intramuscular injections are contraindicated. • Proximal and deep (non-compressible) venous accesses (e.g., jugular, subclavian, brachial, and femoral veins), should be avoided as bleeding can lead to a neurovascular compromise. – The dorsum of hands and feet are the most suitable sites. Factor VIII Deficiency: Prophylaxis & Precautions • Prophylaxis is the standard of care for most patients with severe disease. • Prophylactic replacements (15-40 units/kg) are given every 2-3 days to keep trough levels of 1-2%. The anti-fibrinolytic agent aminocaproic acid (Amicar) can also be given as a prophylactic therapy for oral or dental bleeding. The dose is 25-100 mg/kg every 6-8 h for 7 days. 9/26/2018 16 Optional
- 17. • It is the leading cause of death and can occur spontaneously. • Head trauma or signs of intracranial hemorrhage (headache, irritability, vomiting, seizure, visual problems, focal deficits, stiff neck, or change of consciousness) should be immediately treated with a major-factor infusion prior to diagnostic imaging. • The onset of neurological signs following head trauma may be delayed a few days due to a slowly oozing nature of hemophiliac bleeding. Factor VIII Deficiency: Intracranial Bleeding Bilateral subdural bleeding bleeding dura Epidural (extradural) bleeding bleeding 9/26/2018 17 Optional
- 18. 18
- 19. Inhibitors to Factors VIII and IX • Inhibitors to factors VIII and IX are common in severely affected patients. These antibodies neutralize the activity of infused factors. – Presence of factor inhibitor is suspected if the bleeding does not stop after adequate infusion. – The inhibitor is expressed in Bethesda inhibitor units (BIU). One BIU causes 50% reduction in factor activity. – Patients with low-titer (low responding) inhibitors (<10 BIU) can be treated with increased factor dosing (using 2-3 times the recommended dose). – Patients with high-titer (high responding) inhibitors (>10 BIU), require bypassing products, such as recombinant factor VII (NovoSeven®) or activated prothrombin complex concentrates (FEIBA®). Both preparations may cause thrombosis and disseminated intravascular coagulation. 9/26/2018 19 Optional
- 20. 9/26/2018 20 13-month-old Boy with Abnormal Bruising Normal platelet count & function + normal vWF antigen & activity = intact primary hemostasis Normal PT/INR & TT + prolonged aPTT + low Factor IX activity = Factor IX deficiency (hemophilia B)
- 21. A 2-year-old boy presents to the emergency department with the sudden onset of a large swelling of the left knee. The parents report no history of trauma. He is afebrile and his only complaint is pain in the left knee. His platelet count is 196 x109/L (normal, 150 to 400), aPTT 135.6 sec (normal, 35.2 to 40.4), PT 13.2 sec (normal, 12.2 to 14.6), INR 1.0 (normal, 0.8 to 1.2), and TT 11.4 sec (normal, 9.2 - 12.3). Which one of the following is the MOST likely cause of his findings? A. von Willebrand factor deficiency B. Vitamin K deficiency C. Factor VII deficiency D. Factor VIII deficiency E. Dysfibrinogenemia 219/26/2018
- 22. A 13-month-old boy presents to the emergency department with the sudden onset of a large swelling of the left knee. The parents report no history of significant trauma. He is afebrile and his only complaint is pain in the left knee. His platelet count is 196 x109/L (normal, 150 to 400), aPTT 135.6 sec (normal, 35.2 to 40.4), PT 13.2 sec (normal, 12.2 to 14.6), INR 1.0 (normal, 0.8 to 1.2), and TT 11.4 sec (normal, 9.2 - 12.3). Which one of the following is the MOST appropriate next diagnostic work-up? A. von Willebrand factor antigen and activity B. Factor V and X C. Fibrinogen D. Factors XII, XI, IX and VIII E. Factor VII 229/26/2018
- 23. A 2-year-old boy presents to the emergency department with the sudden onset of a large swelling of the left knee. The parents report no history of trauma. He is afebrile and his only complaint is pain in the left knee. His platelet count is 196 x109/L (normal, 150 to 400), aPTT 135.6 sec (normal, 35.2 to 40.4), PT 13.2 sec (normal, 12.2 to 14.6), INR 1.0 (normal, 0.8 to 1.2), and TT 11.4 sec (normal, 9.2 - 12.3). Factor VIII activity is 2 units/dL (normal, 50 to 100). Which one of the following is the MOST appropriate treatment? A. Fresh frozen plasma B. Cryoprecipitate C. Recombinant factor VIII D. Factor VIII concentrate E. Recombinant factor IX 239/26/2018