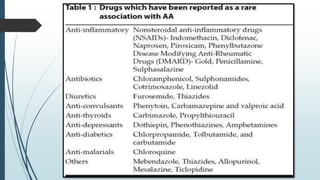
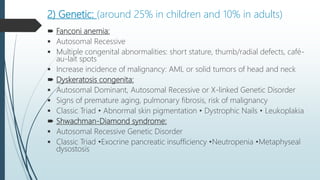
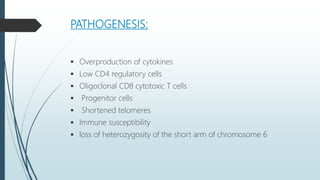
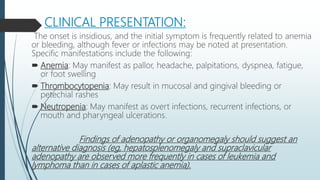
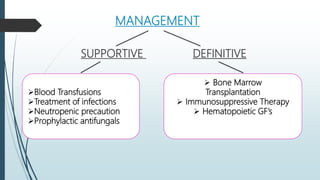
Aplastic anemia is a condition characterized by bone marrow failure leading to pancytopenia and is more common in Asia than in the West, with a peak incidence in childhood and young adulthood. The etiology includes acquired and genetic factors, with the former being predominant, and clinical manifestations often involve anemia, thrombocytopenia, and neutropenia. Management includes supportive care, immunosuppressive therapy, and potential stem cell transplantation, with the prognosis improving significantly over time with advancements in treatment.
































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










