UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Thrombophilias are hypercoagulable conditions that can be acquired or inherited. Most important hypercoagulable conditions =, testing procedures, duration of anticoagulation will be discussed here. Useful for Internal Medicine Boards and Hematology boards. Some aspects on duration of anticoagulation, HIT are high-yield for USMLE exams.
Thrombophilias are hypercoagulable conditions that can be acquired or inherited. Most important hypercoagulable conditions =, testing procedures, duration of anticoagulation will be discussed here. Useful for Internal Medicine Boards and Hematology boards. Some aspects on duration of anticoagulation, HIT are high-yield for USMLE exams.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Autoimmune hemolytic anemia (or autoimmune haemolytic anaemia; AIHA) occurs when antibodies directed against the person's own red blood cells (RBCs) cause them to burst (lyse), leading to insufficient plasma concentration.
Thrombocytopenia is generally defined as platelet count <150 × 109/L. It can occur due to several reasons, like decreased platelet production (e.g., inherited bone marrow failure syndromes, acquired aplastic anemia, leukemia), ineffective platelet production (myelodysplastic syndrome, megaloblastic anemia), increased destruction (ITP, HLH), increased consumption (DIC, TTP, HUS), sequestration (hypersplenism), or may be due to combination of multiple mechanisms described above.
During evaluating a case of thrombocytopenia, the first step is getting a detailed history and doing a proper clinical examination. Then the next step would be checking the other parameters of complete blood count (CBC), especially hemoglobin (Hb) and the total WBC count, complemented by a peripheral smear (PS) examination, which will clear many doubts and will help us pinpointing our diagnostic approach.
Many a times pseudo-thrombocytopenia is encountered in a PS due to platelet clumping by EDTA and can be rectified by collecting blood samples in a citrate or heparin vials or by doing a direct finger prick smear. Any accompanying cytopenia will expand the differential diagnosis and an isolated thrombocytopenia will further narrow it down. Presence of any additional abnormalities of red cells (megaloblasts) or white cells (presence of hyper-segmented neutrophils, atypical lymphoid/myeloid cells) could be present in megaloblastic anemia/MDS, leukemia respectively, while in the presence of fragmented red cells microangiopathic hemolytic anemia should always be ruled out by doing PT and aPTT (DIC, TTP, HUS). In case of isolated thrombocytopenia, the platelet morphology is also important. In many patients in India, especially in eastern region many people have large platelets with their normal platelet count around 100 × 109/L with normal platelet function (Harris platelet syndrome). However, presence of any abnormal platelet morphology along with a low platelet count may indicate a platelet function disorder (large platelets in Bernard Soulier syndrome/ Glanzmann thrombasthenia or small platelets in Wiskott-Aldrich syndrome), especially if encountered in early part of life during evaluation for bleeding symptoms. In case of isolated thrombocytopenia, presence of additional congenital anomalies may point out towards an inherited marrow failure syndrome, e.g. amegakayocytic thrombocytopenia. Exposure to certain drugs may result in isolated low platelet count, e.g., ceftriaxone, piperacillin, heparin. Presence of toxic changes in neutrophils may indicate sepsis related thrombocytopenia. By excluding all these, immune thrombocytopenia (ITP) to be thought as no specific tests or markers are available for this entity and its diagnosis is largely clinical. A further work up complemented by bone marrow examination and in few cases a platelet function test will definitely help in reaching the final diagnosis.
So, summarizing, in the evaluation of a case of thrombocytopenia, all the
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Autoimmune hemolytic anemia (or autoimmune haemolytic anaemia; AIHA) occurs when antibodies directed against the person's own red blood cells (RBCs) cause them to burst (lyse), leading to insufficient plasma concentration.
Thrombocytopenia is generally defined as platelet count <150 × 109/L. It can occur due to several reasons, like decreased platelet production (e.g., inherited bone marrow failure syndromes, acquired aplastic anemia, leukemia), ineffective platelet production (myelodysplastic syndrome, megaloblastic anemia), increased destruction (ITP, HLH), increased consumption (DIC, TTP, HUS), sequestration (hypersplenism), or may be due to combination of multiple mechanisms described above.
During evaluating a case of thrombocytopenia, the first step is getting a detailed history and doing a proper clinical examination. Then the next step would be checking the other parameters of complete blood count (CBC), especially hemoglobin (Hb) and the total WBC count, complemented by a peripheral smear (PS) examination, which will clear many doubts and will help us pinpointing our diagnostic approach.
Many a times pseudo-thrombocytopenia is encountered in a PS due to platelet clumping by EDTA and can be rectified by collecting blood samples in a citrate or heparin vials or by doing a direct finger prick smear. Any accompanying cytopenia will expand the differential diagnosis and an isolated thrombocytopenia will further narrow it down. Presence of any additional abnormalities of red cells (megaloblasts) or white cells (presence of hyper-segmented neutrophils, atypical lymphoid/myeloid cells) could be present in megaloblastic anemia/MDS, leukemia respectively, while in the presence of fragmented red cells microangiopathic hemolytic anemia should always be ruled out by doing PT and aPTT (DIC, TTP, HUS). In case of isolated thrombocytopenia, the platelet morphology is also important. In many patients in India, especially in eastern region many people have large platelets with their normal platelet count around 100 × 109/L with normal platelet function (Harris platelet syndrome). However, presence of any abnormal platelet morphology along with a low platelet count may indicate a platelet function disorder (large platelets in Bernard Soulier syndrome/ Glanzmann thrombasthenia or small platelets in Wiskott-Aldrich syndrome), especially if encountered in early part of life during evaluation for bleeding symptoms. In case of isolated thrombocytopenia, presence of additional congenital anomalies may point out towards an inherited marrow failure syndrome, e.g. amegakayocytic thrombocytopenia. Exposure to certain drugs may result in isolated low platelet count, e.g., ceftriaxone, piperacillin, heparin. Presence of toxic changes in neutrophils may indicate sepsis related thrombocytopenia. By excluding all these, immune thrombocytopenia (ITP) to be thought as no specific tests or markers are available for this entity and its diagnosis is largely clinical. A further work up complemented by bone marrow examination and in few cases a platelet function test will definitely help in reaching the final diagnosis.
So, summarizing, in the evaluation of a case of thrombocytopenia, all the
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Blood banking and transfusion medicine i&iiAbdulKaderSouid
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
UAEU - CMHS - Hematology-Oncology Course - MMH 302 - HONC 320. Education material for medical students - It cover basic principles of hematology and oncology, including CAR-T and gene editing. It can be used for study and review. It illustrates main principles of hematology and oncology.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
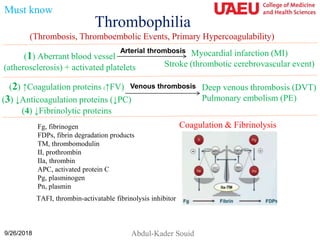
4. Fibrinolysis
Coagulation and fibrinolysis exist as a fine hemostatic balance. Thrombin (IIa) is the central
enzyme in coagulation. It cleaves the soluble fibrinogen (Fg) to insoluble fibrin (FN) clot.
Plasmin (PN) is the central enzyme in fibrinolysis. Plasmin is generated from plasminogen (PG)
by the activity of tissue plasminogen activator (tPA). Plasmin digests the insoluble fibrin (FN)
clot into soluble fibrin degradation products (FDPs). The balance between these two systems is
controlled by natural inhibitors of the cascades. Thrombin generation is inhibited by Protein C
(PC). Plasmin generation is inhibited by “thrombin-activatable fibrinolysis inhibitor” (TAFI).
These two regulatory processes are controlled by the trans-membrane “thrombin-
thrombomodulin (II-TM) complex”. Binding of thrombin to thrombomodulin converts its
substrate specificity from promoting fibrin formation to inhibiting plasmin generation.
Must know
Fg, fibrinogen; FDPs, fibrin degradation products; TM,
thrombomodulin; II, prothrombin; IIa, thrombin; APC,
activated protein C; Pg, plasminogen; Pn, plasmin;
TAFI, thrombin-activatable fibrinolysis inhibitor.
Coagulation & Fibrinolysis
Plasminogen Plasmin
Fibrin
FDPs
tPA (activates)
IIa-TM (inhibits)
5. Harrison's Principles of Internal Medicine, 18e > Chapter 117. Arterial and Venous Thrombosis
Table 117–2 Heritable Causes of Arterial and Venous Thrombosis
A. Arterial Thrombosis
Platelet Receptors:
β3 and α2 integrins
PlA2 polymorphism
Fc(gamma)RIIA
GPIV T13254C polymorphism
GPIb Thrombin receptor PAR-1-5061 → D
Redox Enzymes:
Plasma glutathione peroxidase
H2 promoter haplotype
Endothelial nitric oxide synthase: −786T/C, −922A/G, −1468T/A
Paraoxonase: −107T allele, 192R allele
Homocysteine:
Cystathionine β-synthase 833T → C
5,10-methylene tetrahydrofolate reductase (MTHFR) 677C → T
B. Venous Thrombosis
Coagulant Proteins:
Fibrinogen: −455G/A, −854G/A
Prothrombin (20210G → A)
Protein C Anticoagulant Pathway
Factor V Leiden: 1691G → A (Arg506Gln)
Thrombomodulin: 1481C → T (Ala455Val)
Fibrinolytic Proteins with Known Polymorphisms:
Tissue plasminogen activator (tPA): 7351C/T, 20 099T/C in exon 6, 27 445T/A in intron 10
Plasminogen activator inhibitor (PAI-1): 4G/5G insertion/deletion polymorphism at position −675
9/26/2018
Optional
No need to routinely test for: Homocysteine, factor VIII, MHTFR / XIII polymorphism, & PAI-I
6. ↑Coagulation Proteins
↑Factor V half-life
(mutations in factor V causing resistance to
proteolysis by protein C (protein C
resistance)
↑Factor II (Prothrombin mutation
G20210A)
↑Factor VIII, IX, X, XI
6
↓Anticoagulation Proteins
↓Protein C
↓Protein S
↓Antithrombin (strongest risk)
Heritable Thrombosis
(short list)
9/26/2018
↓Plasminogen
↓Fibrinolytic Proteins
Must know
↑Factor V half-life (important)
The screening test is “activated protein C resistance (APC resistance)” Factor V
mutations; eg, Factor V Leiden (= resistant factor V) = G1691A (Arg506Gln)
↑Homocysteine - MTHFR
polymorphism → arterial thrombosis
(weak effect; no need for testing)
No need to routinely test for: Homocysteine, factor VIII, MHTFR / XIII polymorphism, & PAI-I
7. Activated Protein C (APC) Resistance Assay
(An aPTT-based Assay)
Activated partial thromboplastin time (aPTT)
Citrated plasma + phospholipid + Ca2+ + silica → Measure time to fibrin clot
Citrated plasma + phospholipid + Ca2+ + silica + Activated protein C [APC] → ↑Time to
fibrin clot (a normal response to APC)
Citrated plasma + phospholipid + Ca2+ + silica + Activated protein C [APC} → No
change in the time to form fibrin clot (an abnormal response to APC = APC Resistance)
Protein C inactivates factor V.
Factor V Mutations (e.g., Factor V Leiden)
• They are the most common inherited risk factor for thrombosis.
• Mutation causes factor V to become resistant to proteolysis by protein C.
• It affects 5% of the U.S. white population (heterozygous state).
• Individuals who are heterozygous have a 5-fold ↑risk of venous thrombosis
(especially women who are taking oral contraceptives).
• Individuals who are homozygotes have a 100-fold ↑risk of venous thrombosis.
Must know
8. Protein C Deficiency
The anticoagulant Protein C is activated by a thrombin-
thrombomodulin (IIa-TM) complex on the surface of
endothelial cells. Activated protein C (APC) then binds to
protein S and the resulting protease inactivates factor V,
halting thrombin generation. Homozygous Protein C
deficiency presents early in infancy with purpura fulminans
(shown), which is treated with daily protein C (plasma for
protein S deficiency).
9/26/2018 8
Must know
9. A More Complete Work-up of Thrombosis
9
1. Activated protein C (APC) resistance assay (aPTT-based assay)
2. Factor V Leiden (DNA-based assay, G1691A)
3. Factor II 20210G → A (prothrombin mutation)
4. Protein C & S activity and antigen
5. Antithrombin activity & antigen
6. Homocysteine (blood level)
7. Methyltetrahydrofolate reductase (MTHFR) genetic testing (if ↑homocysteine)
8. Plasminogen activity
9. Tissue plasminogen activator (TPA) antigen
10. Plasminogen activator inhibitor activity (PAI-1)
11. α2–Antiplasmin activity
12. Lipoprotein A (decreases fibrinolysis)
9/26/2018
Optional
10. Vitamin K & Warfarin
• Vitamin K is a fat-soluble vitamin, required for complete synthesis of factors II
(prothrombin), VII, IX, X, Protein C, and Protein S. These six proteins require
vitamin K for the addition of 9-12 γ-carboxyl groups (COO-) at specific glutamate
residues. The resulting carboxylated glutamates mediate Ca2+-dependent binding of
these factors to platelet surface (phospholipids).
• Vitamin K deficiency is caused by (1) Diet short of animal fats (egg yolks, milk, red
meat) and dark green vegetable, (2) Fat malabsorption (biliary obstruction
[cholestasis, direct hyperbilirubinemia], cystic fibrosis), (3) Use of broad-spectrum
antibiotics. Vitamin K deficiency is associated with ↑PT/INR, ↑aPTT, and normal TT.
• Warfarin (coumarin or Coumadin; an anticoagulant) is vitamin K antagonist, which
inhibits the six vitamin K-dependent factors.
• The use of warfarin is challenging because the therapeutic range is narrow (INR =
2.0 to 3.0) and dosing is affected by genetic variation, drug interactions, and diet.
Time spent with a PT/INR above the therapeutic range increases the risk of bleeding,
and time spent below the therapeutic range increases the risk of thromboembolic
complications. Warfarin has a large clinical experience and is highly effective in
reducing the risk of venous and arterial thromboemboli.
Must know
11. Warfarin
• Factor X is the most potent activator of prothrombin and it is the
primary target of anticoagulation by warfarin. Depletion of
factor X prevents prothrombin activation.
• The half-life of factor X is 20-40 h, shorter than that of
prothrombin (60 h). As a result, it takes a few days before the
anticoagulant effects (prothrombin depletion) of warfarin are
fully achieved.
• Thus, for treatment of deep vein thrombosis (DVT), heparin
must be overlapped with warfarin (time to effect = 2-5 days;
half-live about 40 h) for a few days to maintain anticoagulation.
• Reversal of warfarin effect in symptomatic patients include vitamin K (non-
urgent reversal; IV, SC, or oral) and Prothrombin Complex Concentrate (II,
VII, IX, X; for urgent reversal) + vitamain K.
Must know
12. Antithrombotic Agents
Thrombolysis
(recombinant tissue
plasminogen activator, rTPA)
Unfractionated
Heparin
Low Molecular
Weight Heparin
(enoxaparin)
Mechanism
rTPA + Plasminogen →
Plasmin → ↑fibrinolysis
Antithrombin–
dependent
Inactivate Factor X
Indication Threatening thrombi Other thrombi Other thrombi
Dose
IV infusion or injection
directly into the thrombus
IV bolus followed
by infusion
Subcutaneous
every 12 to 24 h
Monitoring ↑D-dimer ↑aPTT
Anti-factor X
activity
Risk of
bleeding
Medium-to-High Low-to-Medium Low
Must know
Warfarin has a large clinical experience and is highly effective in treating
thrombotic events and in reducing the risk of venous and arterial thromboemboli.
The treatment is followed by INR.
Contraindications to thrombolysis include (1) Active bleeding; (2) Intracranial neoplasm; (3) Major
trauma or surgery within 10 days; (4) Severe hypertension; (5) Active seizure; (6) Prematurity (<32
weeks’ gestation); and (7) Platelet count <50 x109/L or fibrinogen <100 mg/dL (2.94 µmol/L).
13. Must Know Pearls
• Activated platelets cause arterial thrombosis.
• ↑Coagulation factor(s) cause venous thrombosis (e.g., ↑factor V, such as factor V Leiden).
– Factor V Leiden = factor V mutation causing resistance to proteolysis by protein C
(Protein C resistance).
• ↓Anticoagulation factor causes venous thrombosis (e.g., ↓Protein C or S).
• ↓Fibrinolytic factor cause venous thrombosis (e.g., ↓plasminogen).
• Antithrombotic therapies include ‘recombinant tissue plasminogen activator’ (rTPA),
warfarin, unfractionated heparin, and low-molecular weight heparin (enoxaparin, inhibits
factor X).
• Avoid oral contraceptives in high-risk thrombotic conditions (positive history of
blood clots).
• Patients with a known risk of thrombosis who are going to be immobilized should
receive prophylactic enoxaparin.
14. Q. A 17-year-old girl presents with left popliteal deep vein thrombosis
(DVT) while taking an estrogen-containing oral contraceptive. Her
maternal family history is positive for DVT.
Which one of the following conditions is the most likely cause of her
precipitated DVT?
A. Protein C deficiency
B. Prothrombin mutation G20210A
C. Antithrombin deficiency
D. Plasminogen deficiency
E. Factor V Leiden (G1691A; Arg506Gln)
9/26/2018 14
15. Required Reading
1. Monagle P, Chan AKC, Goldenberg NA, Ichord RN, Journeycake JM, Nowak-Göttl U,
Vesely SK. Antithrombotic therapy in neonates and children: Antithrombotic Therapy
and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-
Based Clinical Practice Guidelines. Chest. 2012;141:e737S-e801S. doi:
10.1378/chest.11-2308.
2. Harrison's Principles of Internal Medicine, 18e > Chapter 117. Arterial and Venous
Thrombosis
3. Young G, Albisetti M, Bonduel M, et al: Impact of inherited thrombophilia on venous
thromboembolism in children: a systematic review and meta-analysis of observational
studies. Circulation 118:1373–1382, 2008.
4. Daví G, Patrono C: Platelet activation and atherothrombosis. N Engl J Med
13;357:2482, 2007.
5. Mechanisms of thrombus formation. N Engl J Med 28;359:938, 2008.
6. Tapson VF: Acute pulmonary embolism. N Engl J Med 6;358:1037, 2008.
9/26/2018 15
16. Connors JM. Thrombophilia Testing and Venous Thrombosis. N Engl J Med.
2017;377:2298. doi: 10.1056/NEJMc1713797.
9/26/2018 16
17. 9/26/2018 17
Connors JM. Thrombophilia Testing and Venous Thrombosis. N Engl J Med.
2017;377:2298. doi: 10.1056/NEJMc1713797.