Downloaded 225 times

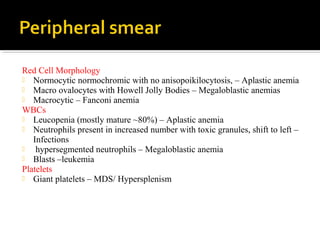
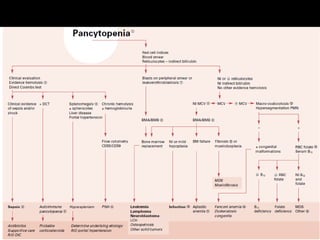


Pancytopenia is a reduction in red blood cells, white blood cells, and platelets in the blood, resulting from various factors including bone marrow failure and immune-mediated destruction. Diagnosis involves clinical examination and specific tests like CBC and bone marrow biopsy, while treatments may include transfusions, corticosteroids, and bone marrow transplants. Congenital causes, such as Fanconi anemia, present with additional clinical features including skeletal and renal abnormalities.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)