Download to read offline




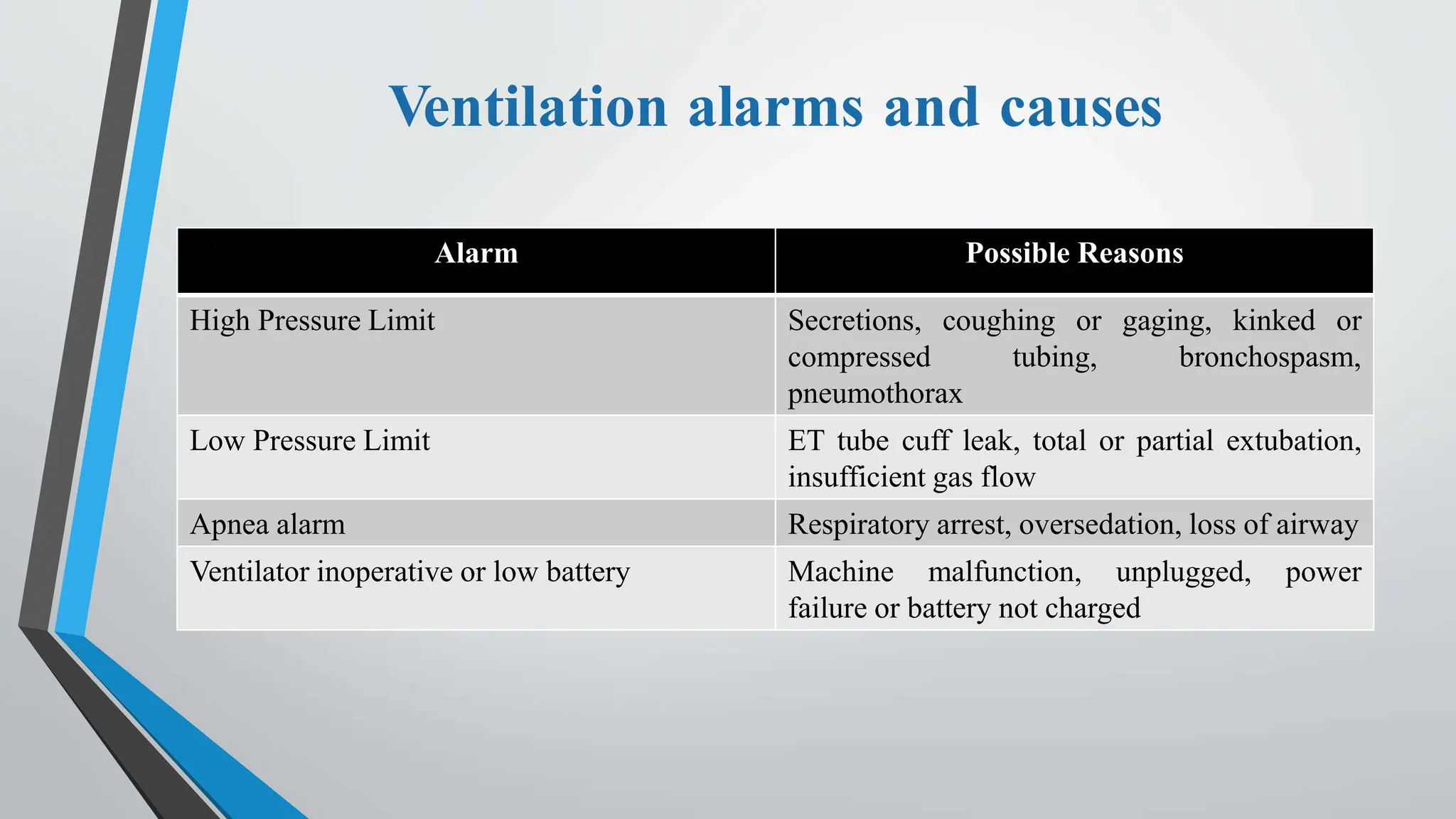
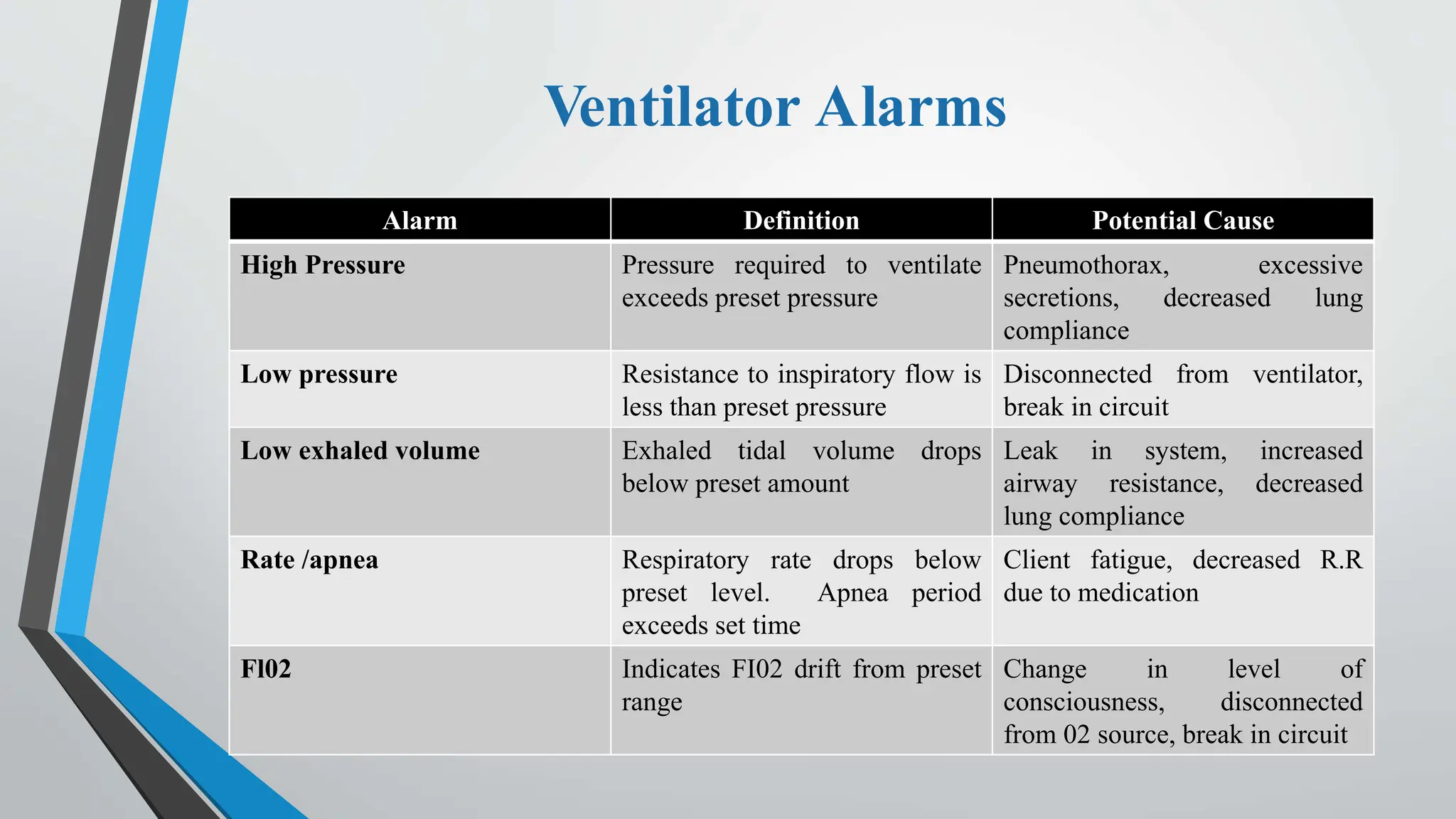









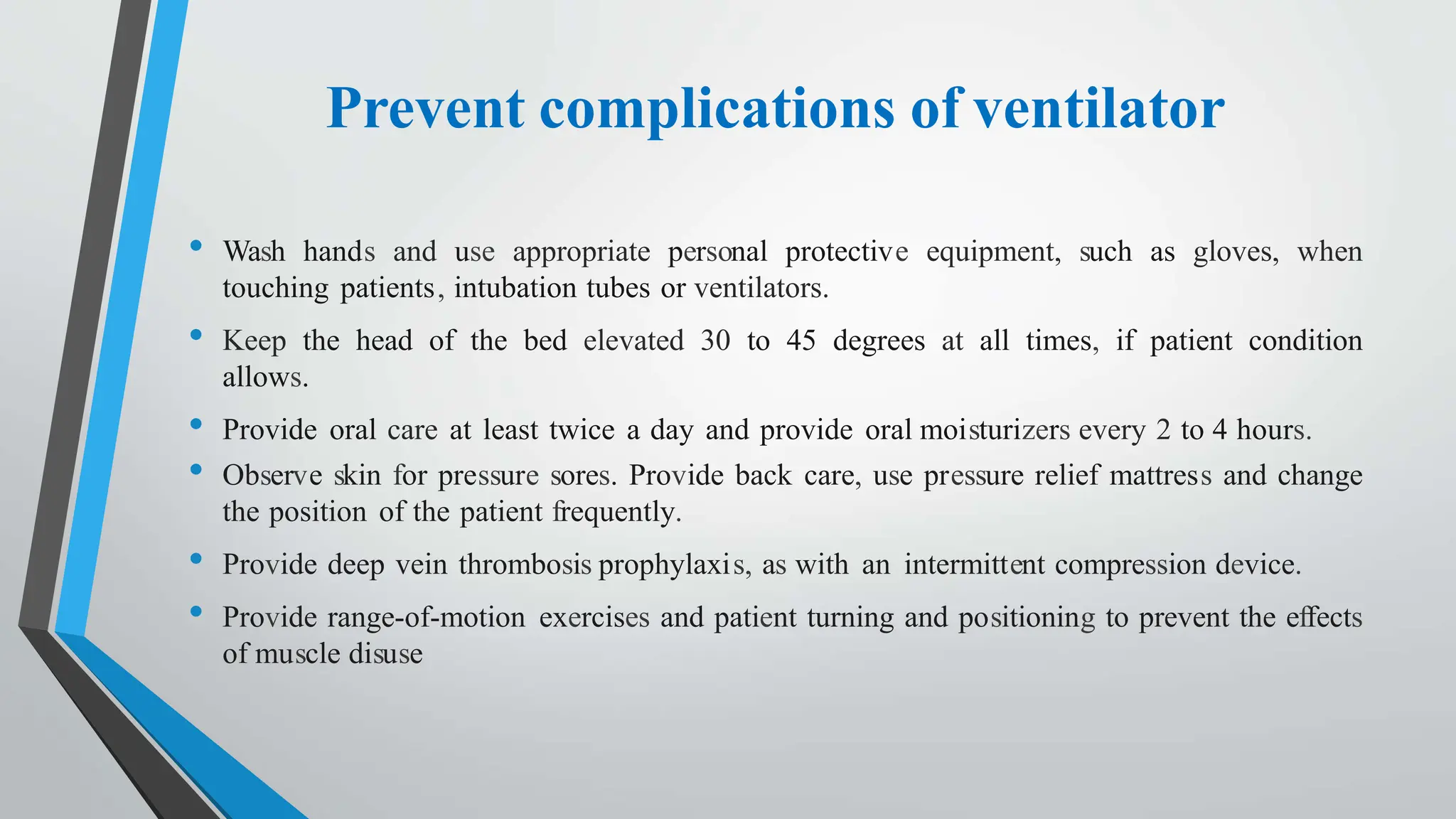


The document outlines key information on ventilator patient care, including definitions of important terms related to respiratory function, types of ventilators, indications for use, modes of ventilation, and potential complications. It emphasizes the importance of monitoring patient status, managing airways, and preventing complications associated with mechanical ventilation. Additionally, the document details best practices for patient hygiene, communication, and hemodynamic stability.















































