WHO guideline
containingrecommendations about
health interventions; clinical, public health
or policy recommendations.
Recommendations are based on
a comprehensive and objective assessment
of the available evidence.
krongdai@gmail.com
6.
free frombias, meet a public health need and
are consistent with the following principles.
The process used to develop is clear,
the reader will be able to see how
a recommendation has been developed,
by whom, and on what basis.
WHO guideline
krongdai@gmail.com
7.
Types of guidelines
•Rapid advice guidelines
• Standard guidelines
• Full guidelines
krongdai@gmail.com
8.
Rapid advice guidelines
Produced within 1–3 months.
May not be supported by full reviews of
the evidence.
Prepared by staff members with external
consultation and peer review.
updated or converted to a standard guideline.
krongdai@gmail.com
9.
Standard guidelines
Usuallytake 9-12 months to complete.
Supported by systematic reviews of the
evidence and one or two meetings group.
May have a specified review-by date of
change of evidence in the topic area.
krongdai@gmail.com
10.
Full guidelines
Wouldbe expected to include
recommendations in relation to all aspects
of the topic.
Fully based on systematic reviews of the
evidence for each aspect.
Likely to take 2-3 years to complete.
krongdai@gmail.com
11.
Compilations of guidelines
Using the Appraisal of Guidelines for
Research and Evaluation (AGREE) tool.
http://www.agreetrust.org/
Some guideline do not require GRC
(Guideline Review Committe) review:
have previously been clear.
krongdai@gmail.com
Adaptations of guidelines
Intended for one setting may be adapted
for use in another.
Adaptations of guidelines must follow
standard GRC procedures.
krongdai@gmail.com
14.
Guidelines prepared
in collaborationwith other organizations
Not by the external group.
No guideline exists or an existing guideline is
outdated.
Met evidence systematically reviewed,
conflicts of interest declared
Reviewing and summarizing evidence should
be consistent.
krongdai@gmail.com
15.
New JBI (JoannaBrigs Institute)
Levels of Evidence
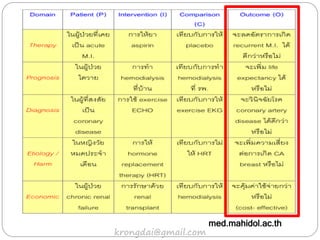
• Level of Evidence for Effectiveness
• Level of Evidence for Diagnosis
• Level of Evidence for Prognosis
• Level of Evidence for Economic evaluations
• Level of Evidence for Meaningfulness
krongdai@gmail.com
16.
New JBI Levelsof Evidence
Level 1 – Experimental Designs
Level 2 – Quasi-experimental Designs
Level 3 – Observational – Analytic Designs
Level 4 – Observational –Descriptive Studies
Level 5 – Expert Opinion and Bench Research
Level of Evidence for Effectiveness
krongdai@gmail.com
17.
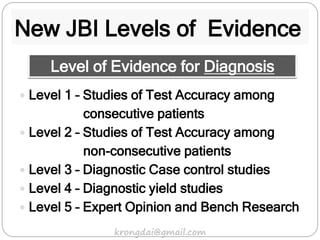
New JBI Levelsof Evidence
Level 1 – Studies of Test Accuracy among
consecutive patients
Level 2 – Studies of Test Accuracy among
non-consecutive patients
Level 3 – Diagnostic Case control studies
Level 4 – Diagnostic yield studies
Level 5 – Expert Opinion and Bench Research
Level of Evidence for Diagnosis
krongdai@gmail.com
18.
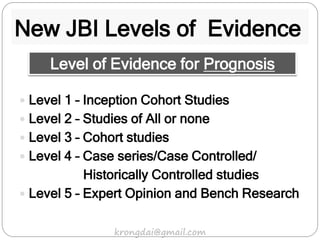
New JBI Levelsof Evidence
Level 1 – Inception Cohort Studies
Level 2 – Studies of All or none
Level 3 – Cohort studies
Level 4 – Case series/Case Controlled/
Historically Controlled studies
Level 5 – Expert Opinion and Bench Research
Level of Evidence for Prognosis
krongdai@gmail.com
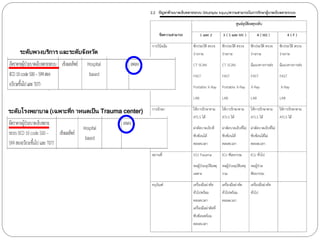
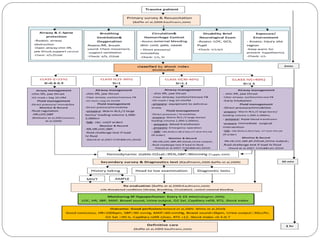
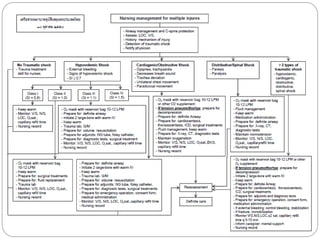
Fast Track Trauma2016
(Minimal Data Set)
• Abdominal injury with shock
• Massive hemothorax
• Cardiac injury
• Traumatic amputation
• EDH/SDH/ICH
42.
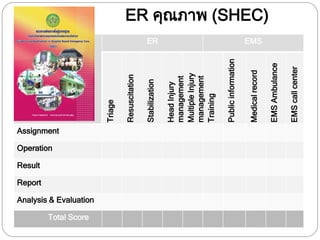
Minimal Data Set
เน้น Fast Tract; Process
ER คุณภาพ
ER to OR
OSCA (out of hospital cardiac arrest)
กาหนดตัวเลขเป็นตัวชี้วัดเวลา.... > 80%
หาตัวเลขกลาง
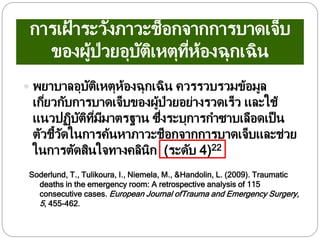
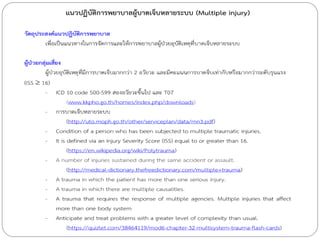
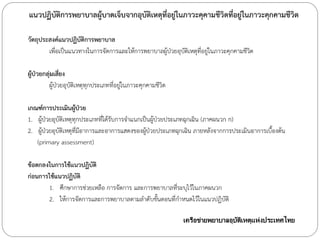
การเฝ้ าระวังภาวะช็อกจากการบาดเจ็บ
ของผู้ป่วยอุบัติเหตุที่ห้องฉุกเฉิน
พยาบาลอุบัติเหตุห้องฉุกเฉินควรรวบรวมข้อมูล
เกี่ยวกับการบาดเจ็บของผู้ป่วยอย่างรวดเร็ว และใช้
แนวปฏิบัติที่มีมาตรฐาน ซึ่งระบุการกาซาบเลือดเป็น
ตัวชี้วัดในการค้นหาภาวะช็อกจากการบาดเจ็บและช่วย
ในการตัดสินใจทางคลินิก (ระดับ 4)22
Soderlund, T., Tulikoura, I., Niemela, M., &Handolin, L. (2009). Traumatic
deaths in the emergency room: A retrospective analysis of 115
consecutive cases. European Journal ofTrauma and Emergency Surgery,
5, 455-462.




















![นำเสนอธนาคารขยะโรงเรียนบ้านห้วยยาง [โหมดความเข้ากันได้]](https://cdn.slidesharecdn.com/ss_thumbnails/random-140825085552-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















































