Downloaded 582 times
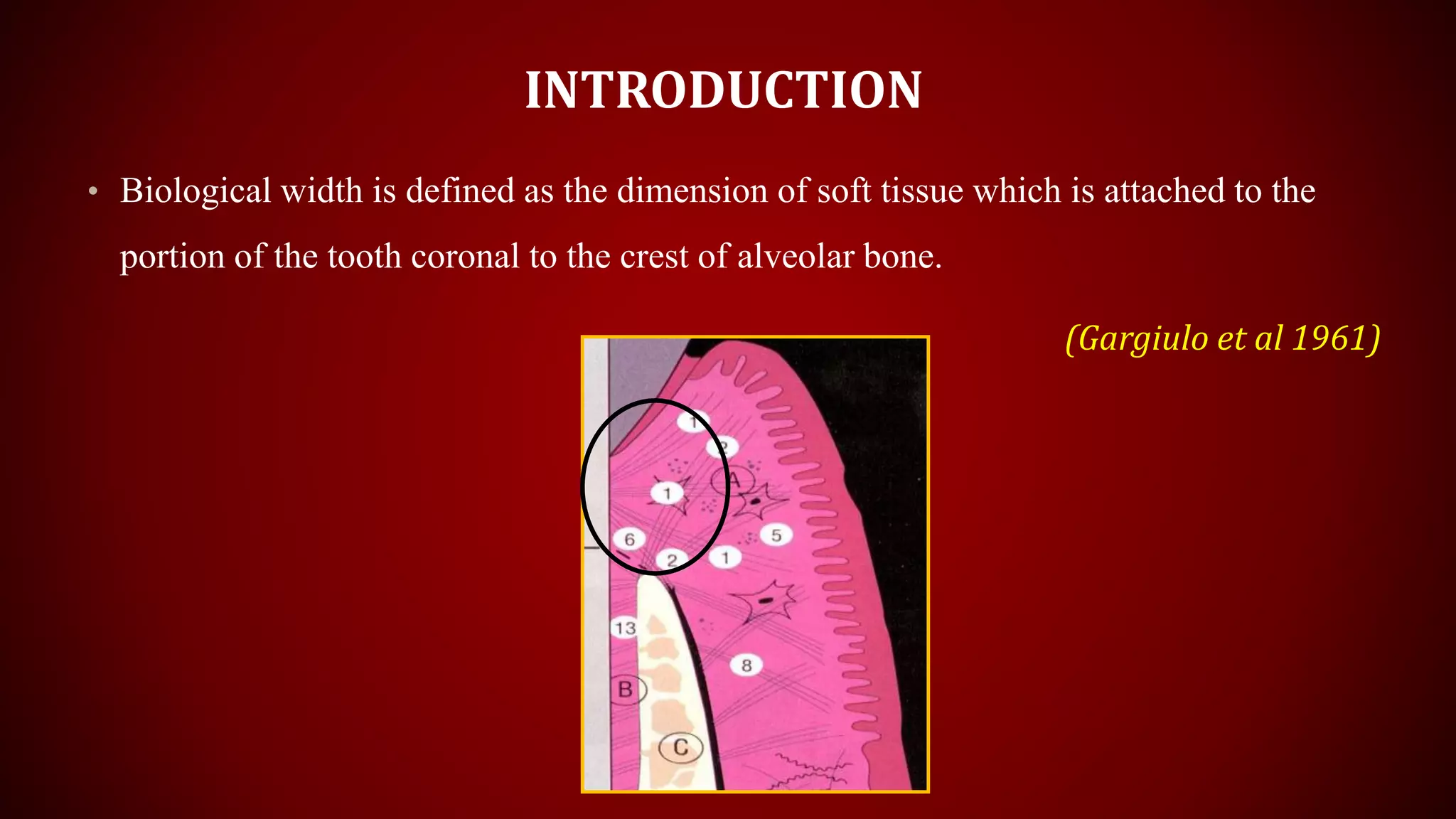


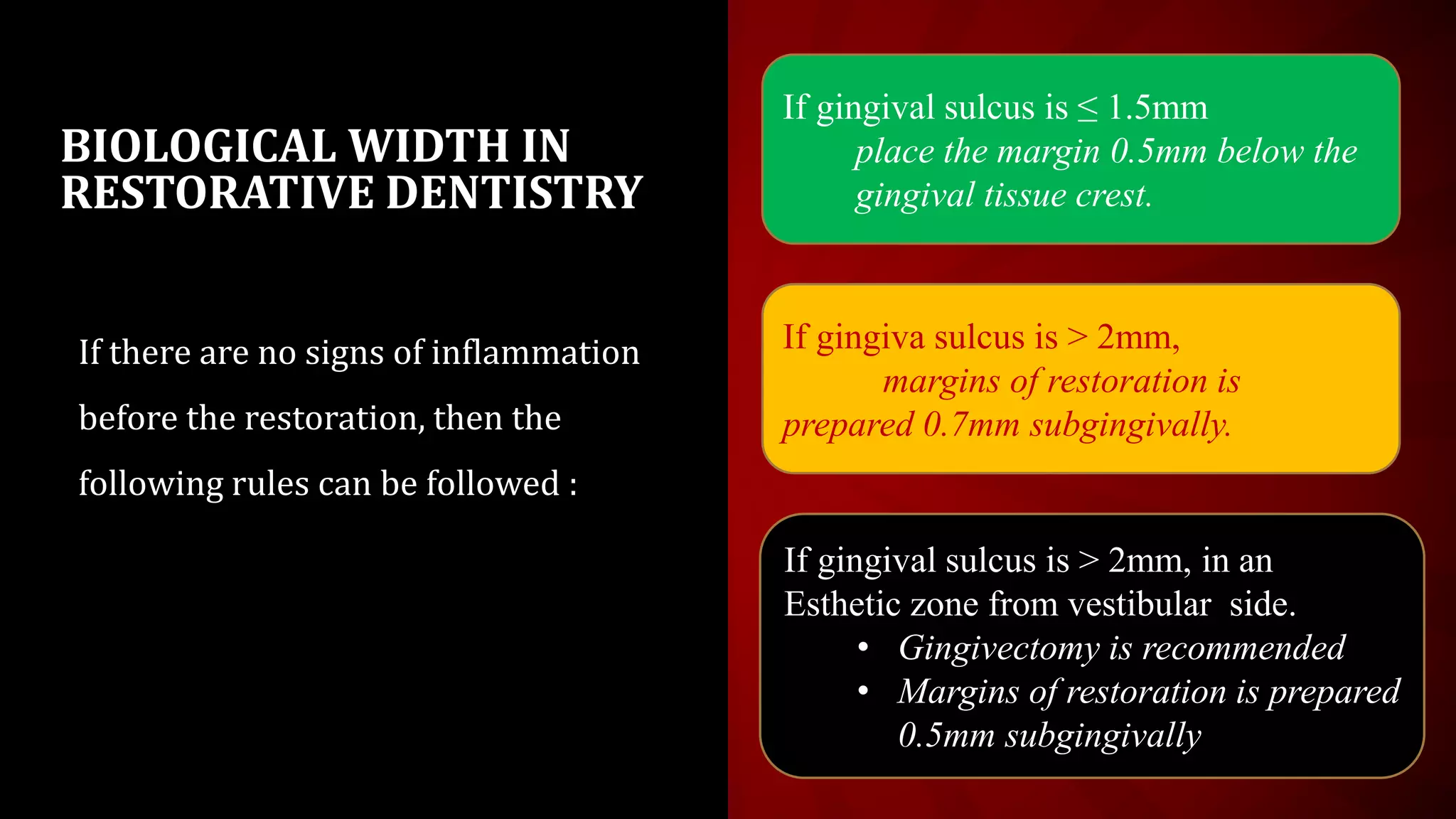


This document discusses biological width, which refers to the dimensions of soft tissue attached to the tooth coronal to the alveolar bone crest. It defines biological width as the connective tissue attachment (1.07mm on average) plus the epithelial attachment (0.97mm on average), totaling 2.04mm. It discusses factors that can lead to biological width violation like subgingival restoration margins and its signs. Methods to evaluate and correct biological width violations like bone sounding, surgical crown lengthening, and forced tooth eruption are also described. The importance of respecting biological width is emphasized in restorative and implant dentistry.