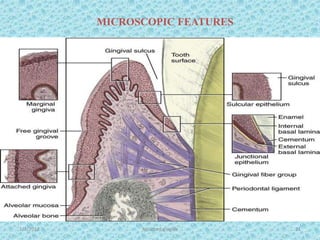
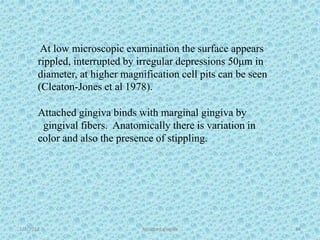
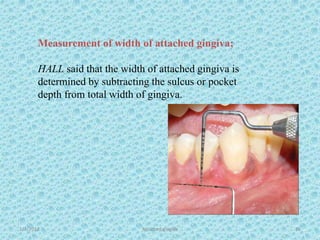
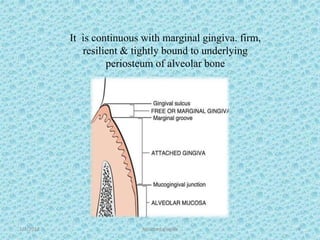
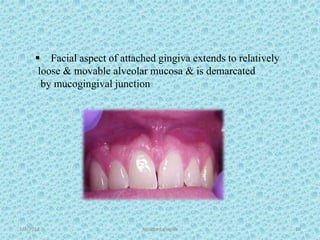
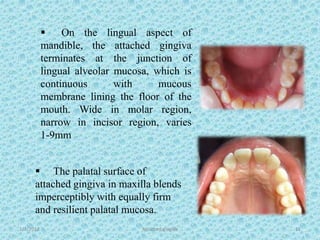
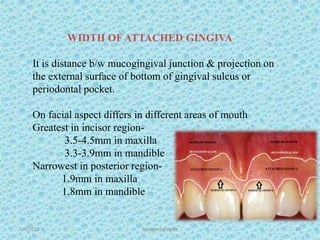
The document discusses attached gingiva, defining it as the portion of gingiva that extends from the base of the gingival crevice to the mucogingival junction. It describes the width and thickness of attached gingiva, noting it varies between 1-9mm wide and has an average thickness of 1.25mm. Microscopically, attached gingiva has a keratinized, cellular epithelium and dense connective tissue. It functions to act as a buffer zone, bear trauma and forces from occlusion, and prevent attachment loss and recession.

![1/7/2018 Attached gingiva 16
presence of an ‘adequate’ zone of gingiva was considered
critical for maintenance of marginal tissue health & for
prevention of continuous loss of connective tissue
attachment.
Inadequate zone of gingiva
1) facilitate subgingival plaque formation
because of improper pocket closure resulting from
mobility of marginal tissue. [Friedman (1962)]
2) favour attachment loss & soft tissue recession
b/c of less tissue resistance to apical spread of
plaque-associated gingival lesion. [stern et al(1976)]](https://image.slidesharecdn.com/attachedgingiva-180107102830/85/ATTACHED-GINGIVA-16-320.jpg)