

![1.Murray C, Lopez A. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries and Risk Factors in 1990 and Projected to 2020.
Cambridge, Massachusetts: Harcourt University Press, 1996.
2.Sackeim HA. The definition and meaning of treatment-resistant depression. Journal of Clinical Psychiatry 2001; 16:10-7.
3.O'Reardon JP, Cristancho P, Peshek A. Vagus nerve Stimulation (VNS) and Treatment of Depression: To the Brainstem and Beyond. Psychiatry 2006; vol 3 -issue 5 - 54-63
4.Groves DA, Brown VJ. Vagal nerve stimulation: a review of its applications and potential mechanisms that mediate its clinical effects. Neuroscience & Biobehavioral Reviews 2005;
29:493-500.
5.Elger G, Hoppe C, Falkai P, Rush AJ, Elger CE. Vagus nerve stimulation is associated with mood improvements in epilepsy patients. Epilepsy Research 2000; 42:203-10.
6.Harden CL, Pulver MC, Ravdin LD, Blagovest N, Halper JP, Labar DR. A pilot study of mood in epilepsy patients treated with vagus nerve stimulation. Epilepsy Behav 2000:93-99.
7.Rush AJ, George MS, Sackeim HA, et al. Vagus nerve stimulation (VNS) for treatment-resistant depressions: a multicenter study.[see comment]. Biological Psychiatry 2000; 47:276-
86.
8.Sackeim HA, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for treatment-resistant depression: efficacy, side effects, and predictors of outcome.
Neuropsychopharmacology 2001; 25:713-28.
9.Rush AJ, Marangell LB, Sackeim HA, et al. Vagus nerve stimulation for treatment-resistant depression: a randomized, controlled acute phase trial. Biological Psychiatry 2005; 58:347-
54.
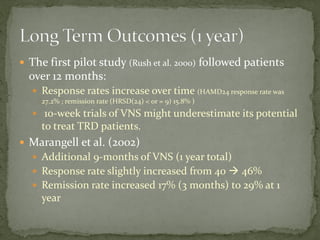
10.Marangell LB, Rush AJ, George MS, et al. Vagus nerve stimulation (VNS) for major depressive episodes: one year outcomes. Biological Psychiatry 2002; 51:280-7.
11.Neurological Devices Panel of Medical Devices Advisory Committee FDA. Report of 17th Meeting. www.fda.gov 2004:1-433.
12.George MS, Rush AJ, Marangell LB, et al. A one-year comparison of vagus nerve stimulation with treatment as usual for treatment-resistant depression. Biological Psychiatry 2005;
58:364-73.
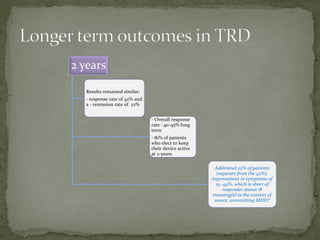
13.Nahas Z, Marangell LB, Husain MM, et al. Two-year outcome of vagus nerve stimulation (VNS) for treatment of major depressive episodes. Journal of Clinical Psychiatry 2005;
66:1097-104.
14.Maisel M. Medical Device Regulation: An introduction for the practicing physician. Annals of Internal Medicine 2004; 146:296-302.
15.Nemeroff CB, Mayberg HS, Krahl SE, et al. VNS Therapy in Treatment-Resistant Depression: Clinical Evidence and Putative Neurobiological Mechanisms.
Neuropsychopharmacology (2006) 31, 1345-1355
16.Lenox RH, Frazer A. Mechanism of action of antidepressants and mood stabilizers (chapter 79). In: Davis KL, Charney D, Coyle JT, Nemeroftt C (eds). Neuropsychopharmacology:
The Fifth Generation of Progress. lippincott Williams & Wilkins: Philadelphia. 2002: 1139-1163
17.George MS, Nahas Z, Bohning DE, et al. Mechanism of action of VNS. clin Neurosci Res 2004 4:71-79
18.Matthews K, Eljamel MS. Vagus nerve stimulation and refractory depression. Br J Psychiatr 2003 183: 181-183
19.Ben-Menachem E. Vagus nerve stimulation, side effects, and long-term safety. Journal of Clinical Neurophysiology 2001; 18:415-8.
20.Rush AJ, Sackeim HA, Marangell LB, et al. Effects of 12 months of vagus nerve stimulation in treatment-resistant depression: a naturalistic study. Biological Psychiatry 2005; 58:355-
63.
21.Rudolph R. Food and Drug Administration Neurological Devices Panel Web site. Executive summary and discussion of the vagus nerve stimulation (VNS) therapy depression
indication clinical data (updated to include information from deficiency letter response). http://www.fda.gov/ohrms/dockets/ac/04/briefing/
4047b1_01_Clinical%20Executive%20Summary-FINAL.pdf., 2005.
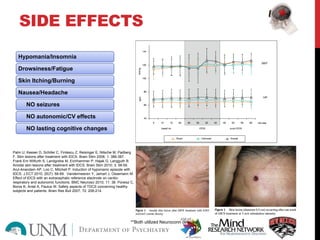
22.Sackeim HA, Keilp JG, Rush AJ, et al. The effects of vagus nerve stimulation on cognitive performance in patients with treatment-resistant depression. Neuropsychiatry,
Neuropsychology, & Behavioral Neurology 2001; 14:53-62
23.Cristancho P, Cristancho MA, Baltuch GH, Thase ME, O’Reardon JP. Effectiveness and Safety of Vagus Nerve stimulation for severe treatment resistant major depression in clinical
practice after FDA approval: Outcomes at one year. J Clin Psychiatry 2011;72 (10):1376- 1382.](https://image.slidesharecdn.com/132626-141113041243-conversion-gate02/85/Transcranial-direct-current-stimulation-64-320.jpg)

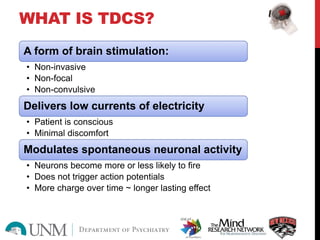
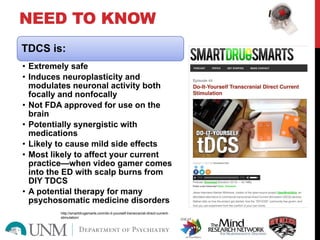
Transracial direct current stimulation (tDCS) is a non-invasive form of brain stimulation that delivers low currents of electricity to modulate neuronal activity. It has been studied as a treatment for conditions such as depression, stroke rehabilitation and cognitive impairment. While generally safe with minor side effects like skin irritation and fatigue, more research is still needed on its efficacy and long term effects before it can be recommended in clinical practice. tDCS holds promise as a treatment to induce neuroplasticity but requires further evaluation in controlled trials.





























































![[Caltech news] beauty and the brain electrical stimulation of the brain make...](https://cdn.slidesharecdn.com/ss_thumbnails/caltechnewsbeautyandthebrainelectricalstimulationofthebrainmakesyouperceivefacesasmoreattractive-130628195845-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)













































