Downloaded 11 times

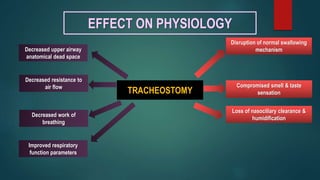


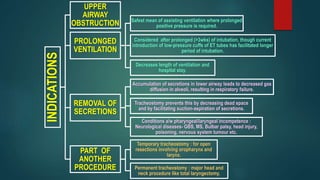

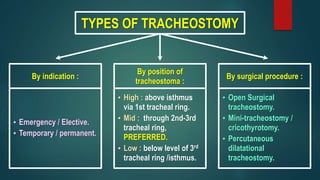

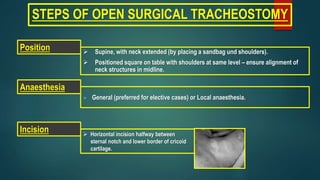
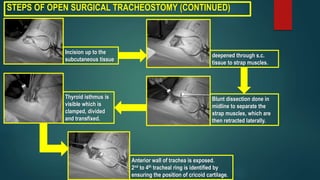



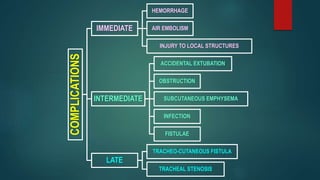
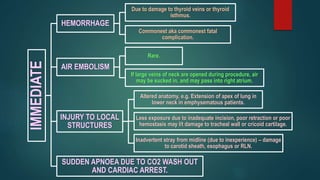
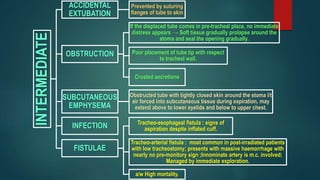

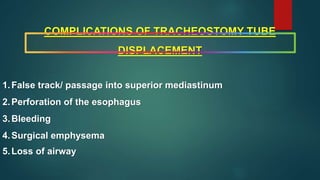
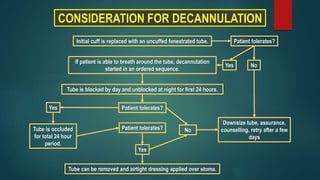
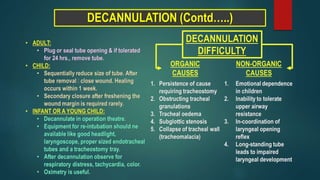








This document provides an overview of tracheostomy, including: - Definitions of tracheostomy and the effect on physiology including disruption of swallowing and improved respiratory function. - Indications such as upper airway obstruction, prolonged ventilation, removal of secretions, and as part of another procedure. - Types including by indication, position, and surgical procedure. - Steps for open surgical tracheostomy and post-operative care. - Potential complications including immediate issues like hemorrhage and injuries, and later issues like tracheo-cutaneous fistula and stenosis. - Considerations for decannulation and tracheostomy tubes including fullers bivalve metallic and jacksons metallic























































































