Downloaded 410 times

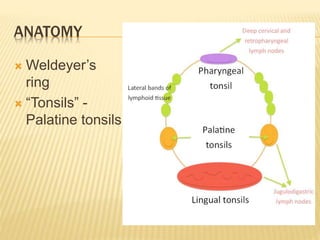





























This document discusses tonsillitis, including the anatomy of the tonsils, types of acute and chronic tonsillitis, indications for tonsillectomy surgery, and complications. It describes how tonsillitis commonly affects school-aged children and presents with symptoms like sore throat and fever. Chronic tonsillitis can lead to complications like peritonsillar abscesses if left untreated. The document outlines the absolute and relative indications for tonsillectomy surgery, including recurrent acute tonsillitis, peritonsillar abscesses, airway obstruction, and suspicion of malignancy.























































































