SVT in pediatrics
•Download as PPT, PDF•
37 likes•12,577 views

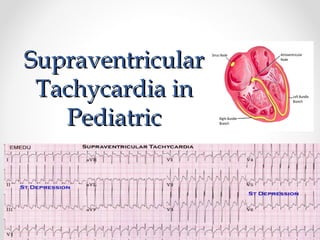
This document discusses supraventricular tachycardia (SVT) in pediatric patients. SVT is the most common abnormal heart rhythm seen in children and the most common arrhythmia requiring treatment. It is usually caused by re-entry mechanisms involving an accessory pathway or the atrioventricular node. Diagnosis involves obtaining an electrocardiogram during episodes to identify P wave patterns. Treatment options include vagal maneuvers, medications like adenosine, calcium channel blockers, or beta blockers, and cardioversion. Radiofrequency ablation can provide a cure for refractory or recurrent cases. Proper diagnosis of the underlying SVT mechanism guides selection of the most appropriate treatment approach.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to SVT in pediatrics
Similar to SVT in pediatrics (20)
Recently uploaded
Recently uploaded (20)
SVT in pediatrics
- 2. Cardiac arrhythmia • is a abnormal electrical activity in the heart • too fast or too slow • regular or irregular. DefinationDefination
- 4. Sinus tachycardia SVT VF VT Atrial fib Atrial flutter Sinus bradycardia Heart block Sinus arrhythmia PAC PVC Tachycardia Bradycardia Irregular
- 5. In structurally normal/ abnormal heart Congenital metabolic disorders of mitochondria SLE Rheumatic fever Myocarditis Toxin (diphtheria) Pro-arrhythmic or anti-arrhythmic drugs Surgical correction of CHD CongenitalCongenital AcquiredAcquired
- 6. Normal Heart RateNormal Heart Rate Age Heart Rate Newborn 120-160 Infant 80- 140 Toddler 1-3 yrs 80- 130 Pre School 3-5yrs 80- 120 School Age 6-12 yrs 70- 110 Adolescent 13+ 60- 100
- 7. Range from Completely asymptomatic Loss of consciousness Sudden cardiac death In infants Lethargy Poor feeding Irritability Cardiac failure Underlying congenital heart disease In children Palpitation Syncope Dizziness Chronic fatigue Shortness of breath Chest discomfort
- 8. History Symptoms Frequency and length of episode Onset and triggers Any underlying disease Medications o Triggering factor o Used for underlying cardiac disease Evaluation Child withEvaluation Child with ArrhythmiaArrhythmia
- 9. DiagnosisDiagnosis Always do- 12 Lead ECG!!!!! -During tachycardia -In sinus rhythm
- 10. Diagnostic methodsDiagnostic methods • Always • Always • Always record a rhythm strip during any intervention (adenosine, cardioversion, Valsalva, etc.)
- 11. Diagnostic methodsDiagnostic methods • Holter • Event recorder • Exercise ECG • Post-op atrial/ventricular pacing wires • Esophageal pacing leads • Adenosine can be diagnostic • Invasive electrophysiology study
- 12. Sinus RhythmSinus Rhythm Every QRS complex is preceded by a P wave and every P wave must be followed by a QRS The P wave morphology and axis must be normal and PR interval will usually be normal for that age
- 14. Sinus ArrhythmiaSinus Arrhythmia Most common irregularity of heart rhythm seen in children Normal variant Heart rate increases during inspiration and decreases during expiration
- 15. Sinus ArrhythmiaSinus Arrhythmia Normal phasic variation of heart rate with respiration Variable P-P intervals No treatment needed
- 16. TachyarrhythmiaTachyarrhythmia • Supraventricular Tachycardia • Ventricular Tachycardia
- 17. Basic Mechanism ofBasic Mechanism of TachycardiaTachycardia 1. Re- entry – most common 2. Automaticity 3. Triggered activity - rare
- 18. Re – entry TachycardiaRe – entry Tachycardia
- 20. SVTSVT Most common abnormal tachycardia seen in pediatric practice Most common arrhythmia requiring treatment in pediatric population Most frequent age presentation: 1st 3 months of life 2nd peaks @ 8-10 and in adolescence
- 21. SVTSVT Commonest mechanism – re-entry - Accessory pathway – 80% -AV nodal re-entry – 20% -Younger age – accessory pathway -Older age - AVNRT
- 22. SVT - classificationSVT - classification AV node Dependent Tachycardia AV Node independent Tachycardia AVRT - concealed pathway - manifest pathway -WPW syndrome Sinus node reentrant Tachycardia AVNRT - Typical ( slow-fast) - Atypical (Fast-slow) Atrial Tachycardia - Focal atrial tachycardia - Multifocal atrial tachycardia Juctional Ectopic Tachycardia ( JET) Atrial Flutter Permanent Juctional Reciprocating Tachycardia ( PJRT) Atrial Fibrillation
- 23. P wave in TachycardiaP wave in Tachycardia - Important to identify p wave during the tachycardia - Helps to guide types of SVT - No p wave - Short RP tachycardia - Long RP tachycardia
- 24. P wave in TachycardiaP wave in Tachycardia No visible p Wave, narrow complex - AVNRT
- 25. P wave in Tachycardia –P wave in Tachycardia – Short RPShort RP - AVRT - Typical AVNRT
- 26. P wave in Tachycardia –P wave in Tachycardia – Short RPShort RP
- 27. P wave in Tachycardia –P wave in Tachycardia – Long RPLong RP - Atypical AVNRT - PJRT - Atrial tachycardia - Sinus tachycardia - sinus node tachycardia
- 28. P wave in Tachycardia –P wave in Tachycardia – Long RPLong RP
- 29. What's Next?What's Next? LOOK FOR THE R-R interval - regular - irregular Gives clues on types of SVT
- 31. ANRT - P wave on STANRT - P wave on ST segmentsegment Regular R-R intervalRegular R-R interval
- 32. AVNRT - p wave absent orAVNRT - p wave absent or pseudo r wave on VIpseudo r wave on VI Regular R-R intervalRegular R-R interval
- 33. AET - Long RP tachycardiaAET - Long RP tachycardia with abnormal p wavewith abnormal p wave morphologymorphology Regular R-R intervalRegular R-R interval
- 34. PJRT -Long RP tachycardiaPJRT -Long RP tachycardia with abnormal p wavewith abnormal p wave inverted lead II,III,aVFinverted lead II,III,aVF Regular R-R intervalRegular R-R interval
- 35. Atrial flutter – saw toothAtrial flutter – saw tooth baselinebaseline
- 36. MET – Irregular TachycardiaMET – Irregular Tachycardia Long RPLong RP different p wavedifferent p wave morphologymorphology
- 37. JET – Irregular R-R intervalJET – Irregular R-R interval p wave with VA dissociationp wave with VA dissociation
- 38. ManagementManagement Treatment Option SVT Termination 1.Vagal maneuvers 2.Anti arrhythmic drugs ( IV or Oral ) 3.Electrical Termination - DC cardioversion - Endocardial pacing - Trans Esophageal pacing
- 40. ManagementManagement Vagal Maneuvers 1.Smaller childrens and infants - Ice cold facecloth to the face - Stimulate the vagal response 1.Older childrens - carotid massage - Valsalva technique
- 41. Management - IVManagement - IV AdenosineAdenosine • Diagnostic and therapeutic • Given via central line better than peripheral • Short half life • 100-500mcg/kg given rapid IV push • ALWAYS!!! Record rhythm strip during adenosine
- 45. SVT TreatmentSVT Treatment 1. IV Verapamil – older childrens 0.1mg/kg - Contraindicated in < 4 yrs old and in WPW syndrome 1. Digoxin – useful in infants - Contraindicated in WPW 1. IV propranolol 0.1mg/kg 2. IV Flecanaide 0.5-2mg/kg 3. IV amiodarone 5mg/kg in 30min and 5- 15mcg/kg/min 4. Cardioversion 0.5-2J/kg
- 46. Management- PreventionManagement- Prevention 1.No treatment 2.Anti Arrhythmic drug 3.Radiofrequency ablation
- 47. Management - PreventionManagement - Prevention No Treatment -Infrequent eposides -Explain -Educate on valsalva -PRN treatment in ED
- 48. Management - PreventionManagement - Prevention
- 49. Management - PreventionManagement - Prevention
- 50. Treatment OptionsTreatment Options 1. AV node - Digoxin - Class II – beta blockers - Class III – Amiodarone - Class IV – Verapamil 1. Accessory pathway - Class 1C – Flecanaide - Class III – Amiodarone - WPW- No Verapamil or Digoxin
- 51. Management - PreventionManagement - Prevention Radiofrequency Ablation – invasive procedure - Curative -Older children's -Incessant SVT- PJRT -Symptomatic SVT -Drug refractory SVT -WPW with symptomatic
- 52. SummarySummary • SVT generally well tolerated, life threatening is uncommon • Record 12 lead ECG during arrhythmia • Record rhythm strip during any intervention • ECG clue for diagnosis – wide or narrow complex, p wave relationship to QRS and regular or irregular rhythm • Proper diagnosis can guide appropriate Tx