1) Tonsillitis is an inflammation of the palatine tonsils caused by bacterial or viral infection. It is commonly found in children and young adults.
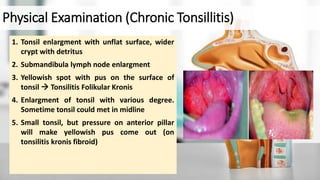
2) Symptoms include sore throat, fever, swollen tonsils, and pain when swallowing. Chronic tonsillitis presents with recurrent sore throats.
3) Diagnosis involves examining the throat for swollen, red tonsils and potentially testing for strep infection. The severity of tonsil enlargement is graded on a scale from T1 to T4.


































![• Adams, G. L., Boies, L. R., and Higler, P. A., 2012. ‘BOIES Buku Ajar Penyakit THT’. 6 ed. Philadelphia: Boeis Fundmentals Of Otolaryngology.
• Anderson, J. and Paterek, E., 2021. Tonsillitis. [online] Ncbi.nlm.nih.gov. Available at: [Accessed 04 February 2022].
• Anniko, M., Bernal-Sprekelsen, M., Bonkowsky., Bradley, P., Lurato, S., 2018. ‘Otorhinolaryngology, Head and Neck Surgery’. Springer
• Basuki, S., W. et al., 2020. ‘Tonsilitis’. Publikasi Ilmiah Universitas Muhammadiyah Surakarta, 5(1), pp. 483-494.
• Bird, J., Biggs, T. and King, E., 2014. ‘Controversies in the management of acute tonsillitis: an evidence-based review’. Clinical Otolaryngology, 39(6), pp.368-374.
• Bonkowsky, V. & Gerdemann, P., 2018. Oropharynx and Hypopharynx in ‘Otorhinolaryngology, Head and Neck Surgery’. Springer International Publisher
• Depkes RI. ‘Tonsilektomi pada anak dan dewasa.Cermin Dunia Kedokteran’; Jakarta. 2013; 155:87-91.
• Dhingra, P.L., Dhingra, D., Dhingra, S, 2017. ‘Diseases of Ear, Nose and Throat, and Head & Neck Surgery’. 6th ed., New Delhi, Elsevier, pp. 291-295.
• Feng, B., Feng, Y., Zhou, X., Mu, Z., Fang, J., 2021. Common Pharyngeal Disease in ‘Practical Otorhinolaryngology-Head and Neck Surgery’. Springer International Publisher
• Hazarika, P., Nayak, D.R., Balakrishnan, R., 2018. ‘Textbook Of Ear Nose Throat and Head and Neck Surgery Clinical AND Practical’. 3rd Ed. CBS Publisher and Distributors
• Hidalgo, J. A. & Vazquez, J. A., 2020. Candidiasis. [Online]. Available at: https://emedicine.medscape.com/article/213853-overview. [Accesed at 9 February 2022]
• Hui, C. S., 2015. ‘Prevalensi Tonsilitis di Rumah Sakit Umum Pusat Haji Adam Malik Tahun 2015’, Repository USU.
• Khan, D., Hamraz, M., Khattak, A., Ali, I., Khalil, U. and Khan, Z., 2019. ‘The analysis of risk factors associated with tonsillitis: a case study of district Mardan, Pakistan’. Journal of the Pakistan Medical Association, p.1169- 1171.
• Kraft, K., C, C., Gerogalas, Tolley, N. & Narula, A. 2014, ‘Tonsillitis’, MMW Fortschritte der Medizin, 153(32–34), p. 18. doi: 10.1007/BF03368657
• Kumar et al. 2010. ‘Pathologic Basic of Disease’. 8th Edition. Philadelphia : Elsevier.
• Marchak, A., 2018. Tonsillitis: Pathogenesis and clinical findings | Calgary Guide. [online] The Calgary Guide to Understanding Disease. Available at: [Accessed 04 February 2022].
• Masters, K., Zezoff, D. and Lasrado, S., 2021. Anatomy, Head and Neck, Tonsils. [online] Ncbi.nlm.nih.gov. Available at: https://www.ncbi.nlm.nih.gov/books/NBK539792/ [Accessed 04 February 2022].
• Mu, Z., & Fang, J., 2020. ‘Practical Otorhinolaryngology - Head and Neck Surgery’. https://doi.org/10.1007/978-981-13-7993-2
• Onerci, T. M. & Altunay, Z. O., 2021. ‘Diagnosis in Otorhinolaryngology’. 2nd Eds. Springer International Publisher
• Pappas, P. G., Kauffman, C.A., Andes, D. R., Clancy, C.J., Marr, K.A., Ostrosky-Zeichner, L. et al, 2015. ‘Clinical Practice Guidline for the Management of Candidiasis: 2016 Update by the Infectious Disease of Society of America’.
Clinical Infectious Disease. USA.
Reference](https://image.slidesharecdn.com/referat-tonsilitis-ramamaleakhisaragih-220218032515/85/Tonsillitis-41-320.jpg)
![• Plank, L., 2016. ‘Acute Tonsilitis’. Springer International Publishing Switzerland
• Rusmajono & Soepardi, E.A., 2011 Faringitis, Tonsilitis, dan Hipertrofi Adenoid in ‘Buku Ajar Ilmu Kesehatan Telinga Hidung Tenggorok Kepala Leher’. 6th ed.
Fakultas Kedokteran Universitas Indonesia.
• Sari, L. T., Ambarwati & Kusumawati, Y. 2014, ‘Faktor pencetus tonsilitis pada anak usia 5-6 tahun di wilayah kerja Puskesmas Bayat Kabupaten Klaten’.
• Sidell, D. and L. Shapiro, N., 2012. ‘Acute Tonsillitis’. Infectious Disorders - Drug Targets, 12(4), pp.271-276.
• Stephen, J.M. & Anand, J., 2019. ‘Acute Necrotizing Ulcerative Gingivitis Empiric Therapy’. [Online]. Available at:
https://emedicine.medscape.com/article/2028117-overview#a1. [Accesed at 09 February 2022].
• Van Gijn, D.R. & Dunne, J., 2019. ‘Oxford Handbook of Head and Neck Anatomy’. 1st ed. Oxford University Press
• Walijee, H., Patel, C., Brahmabhatt, P. and Krishnan, M., 2017. ‘Tonsillitis’. InnovAiT: Education and inspiration for general practice, 10(10), pp.577-584.
• Windfuhr, J., Toepfner, N., Steffen, G., Waldfahrer, F. and Berner, R., 2016. ‘Clinical practice guideline: tonsillitis I. Diagnostics and nonsurgical management’.
European Archives of Oto-Rhino-Laryngology, 273(4), pp.973-987.
• Zhou, X. & Bi, X., 2020. Applied Anatomy and Physiology of Pharynx in ‘Practical Otorhinolaryngology-Diagnosis and Treatment’. Springer Nature Singapore. China
Reference](https://image.slidesharecdn.com/referat-tonsilitis-ramamaleakhisaragih-220218032515/85/Tonsillitis-42-320.jpg)




































































