Downloaded 222 times


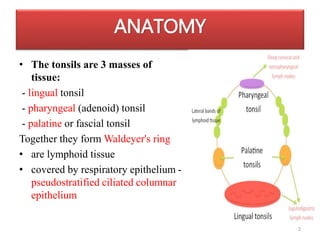




The tonsils are lymphoid tissue located in Waldeyer's ring in the pharynx. They help defend against pathogens and produce antibodies. Tonsillitis can be acute, caused by viruses or streptococcus bacteria, or chronic with recurrent infections. Chronic tonsillitis presents with bad breath, sore throat, and debris in crypts. Large tonsils and adenoids can obstruct the airway and cause sleep issues. Tonsillectomy and/or adenoidectomy may be recommended for recurrent infections, airway obstruction, or chronic tonsillitis resistant to other treatments. Complications can include abscesses.











































































































