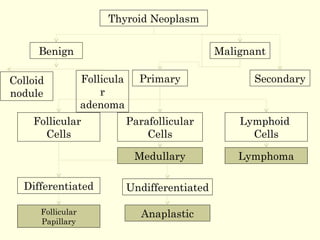
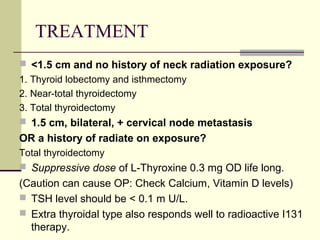
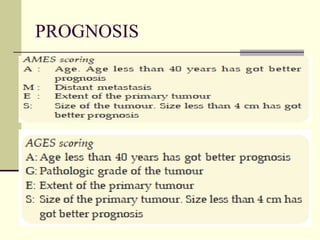
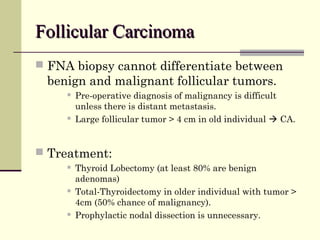
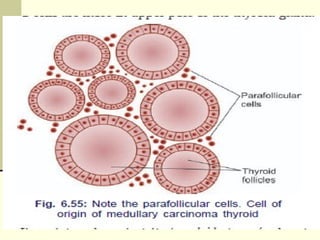
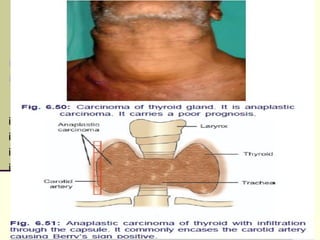
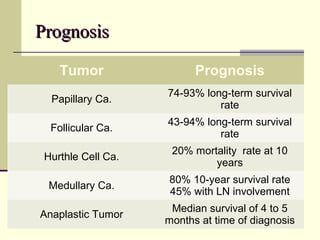
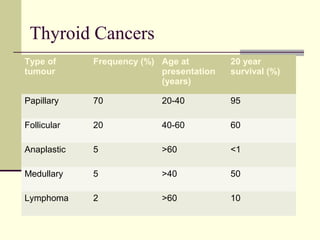
Thyroid cancers are the most common endocrine malignancies, with papillary carcinoma being the most frequent type at 60% of cases. Papillary carcinoma commonly presents in younger females and has a good prognosis with a 95% 20-year survival rate. Medullary carcinoma is a rare but aggressive type associated with genetic syndromes. Anaplastic carcinoma is the most lethal type with median survival of only 4-5 months. Treatment options depend on tumor size and extent, and may include thyroid lobectomy, total thyroidectomy, radioactive iodine, chemotherapy, or external beam radiation.








































![Thyroid carcinoma final [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidcarcinomafinalpart2-161126043433-thumbnail.jpg?width=640&height=640&fit=bounds)














































