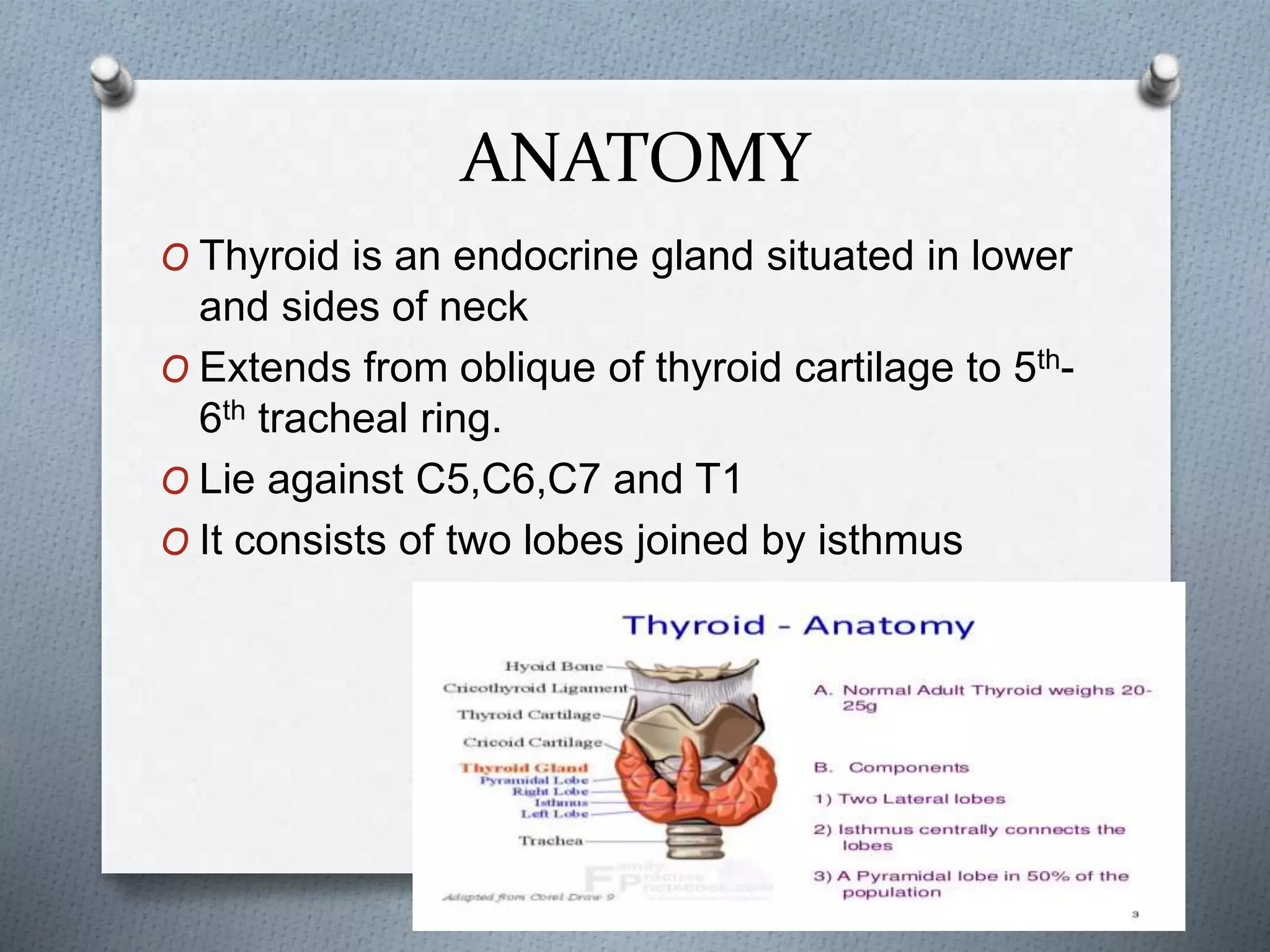
1) The thyroid gland is located in the lower front of the neck and produces thyroid hormones that regulate metabolism.
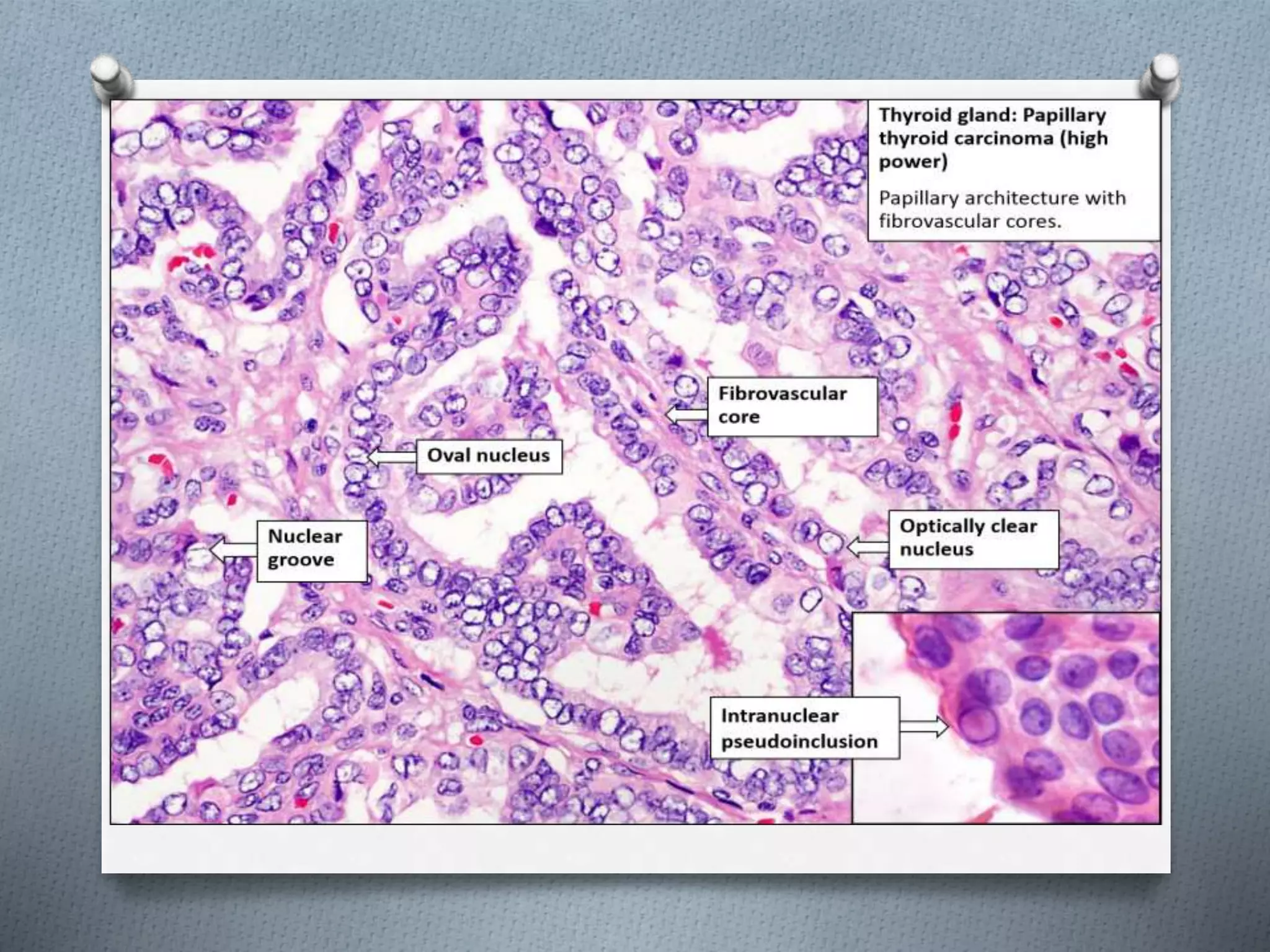
2) The main types of thyroid cancer are papillary carcinoma (60%), follicular carcinoma (20%), anaplastic carcinoma (10%), and medullary carcinoma (5%).
3) Diagnosis involves blood tests, ultrasound, and biopsy. Treatment options include surgery, radioactive iodine treatment, and thyroid hormone suppression. Prognosis is generally good if cancer is detected and treated early.














































![Thyroid carcinoma final [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidcarcinomafinalpart2-161126043433-thumbnail.jpg?width=640&height=640&fit=bounds)





































