This document discusses diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS), two serious complications of diabetes. It defines DKA as hyperglycemia, ketosis, and acidosis, while defining HHS as hyperglycemia, hyperosmolarity, and altered mental status. It then provides further details on the pathogenesis, diagnostic evaluation, treatment, and monitoring of patients with DKA or HHS. Hypoglycemia is also briefly discussed.


![DKA = 3 letters= triad of D K A
Diabetic
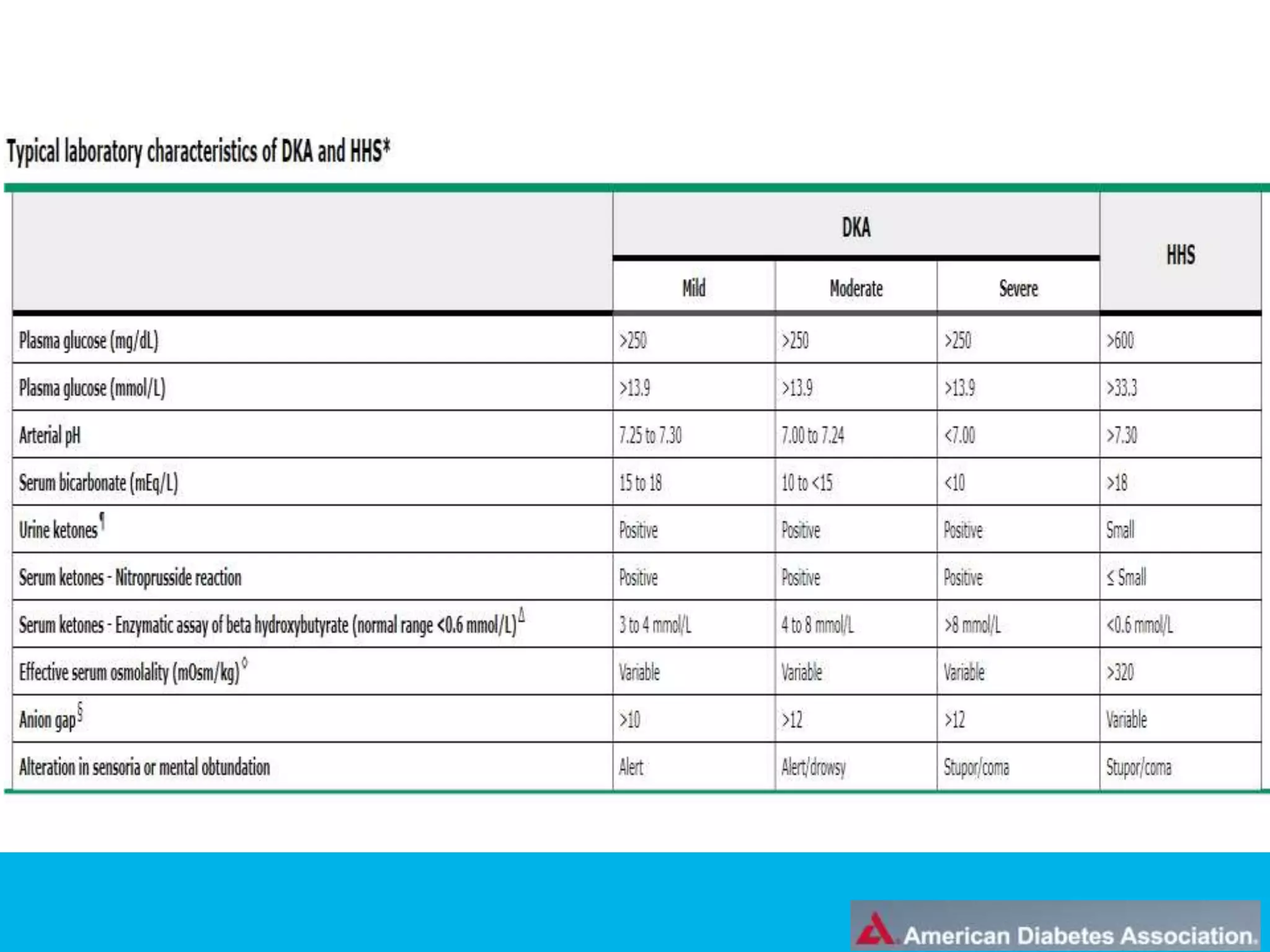
glucose >250 mg/dL
Keto
ketones – both in urine and in serum
acetoacetate, acetone, betahydroxybutyrate
fruity smell.
If the Ketone level is below 0.6 mmol/L is normal.
The person with a reading above 1.5 mmol/L indicate a greater
risk for developing Ketoacidosis (DKA).
Acidosis
Increased anion gap AG=[(Na)-(Hco3+CL)],metabolic acidosis;
HCO3-
<15, pH<7.30
The normal blood pH is tightly regulated between 7.35 and 7.45.](https://image.slidesharecdn.com/dmemergencies-dpg-190121142705/75/DIABETIC-EMERGENCIES-DKA-HONK-HYPOGLYCEMIA-5-2048.jpg)
















![Treatment
For asymptomatic or symptomatic hypoglycemia ,ingest
carbohydrates. 15 to 20 grams of oral glucose is
typically sufficient. Glucose may be ingested in the form
of tablets, juice, milk,
glucagon(0.5 to 1.0) mg given as a subcutaneous or
intramuscular injection. If difficult IV access .(or at
home)
EDUCATION .
IV dextrose (25 g of 50 percent glucose [dextrose]) can
be administered to treat hypoglycemia in patients with
impaired consciousness and established IV access
(typically in hospital).](https://image.slidesharecdn.com/dmemergencies-dpg-190121142705/75/DIABETIC-EMERGENCIES-DKA-HONK-HYPOGLYCEMIA-25-2048.jpg)





































![Management of diabitic_keto_acidosis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/management-of-diabitic-ketoacidosis-5b1-5d-140226042211-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


















































