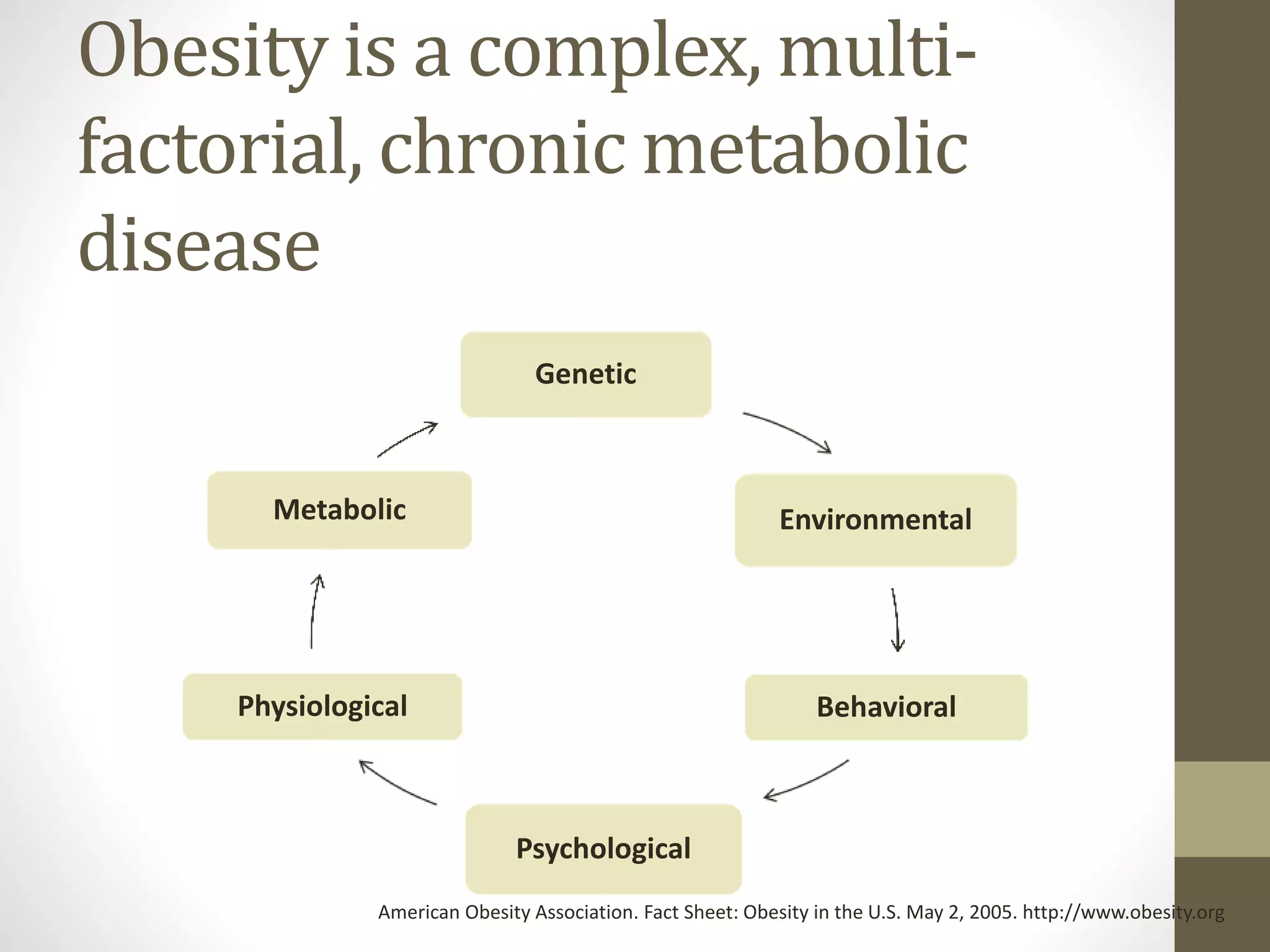
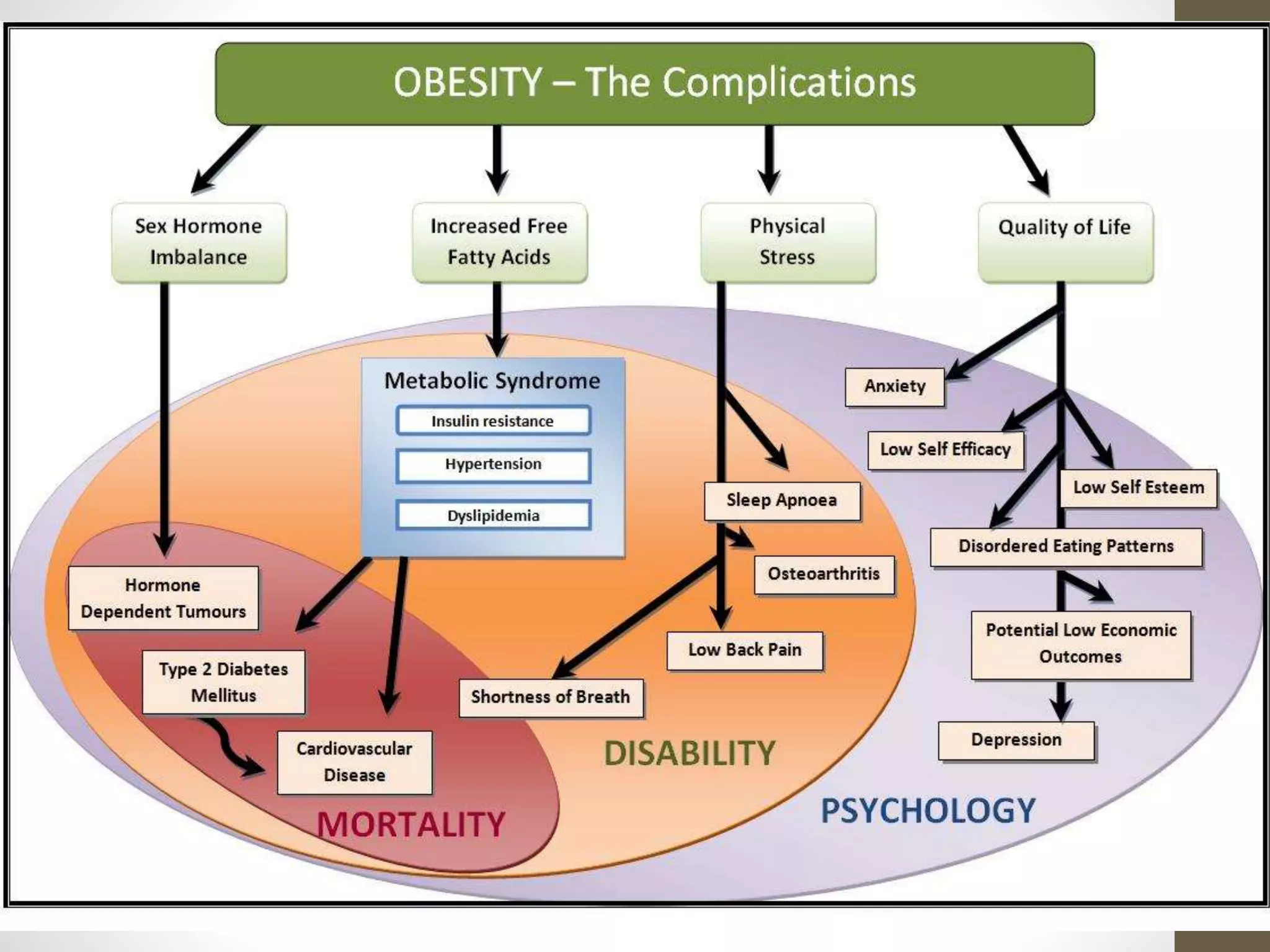
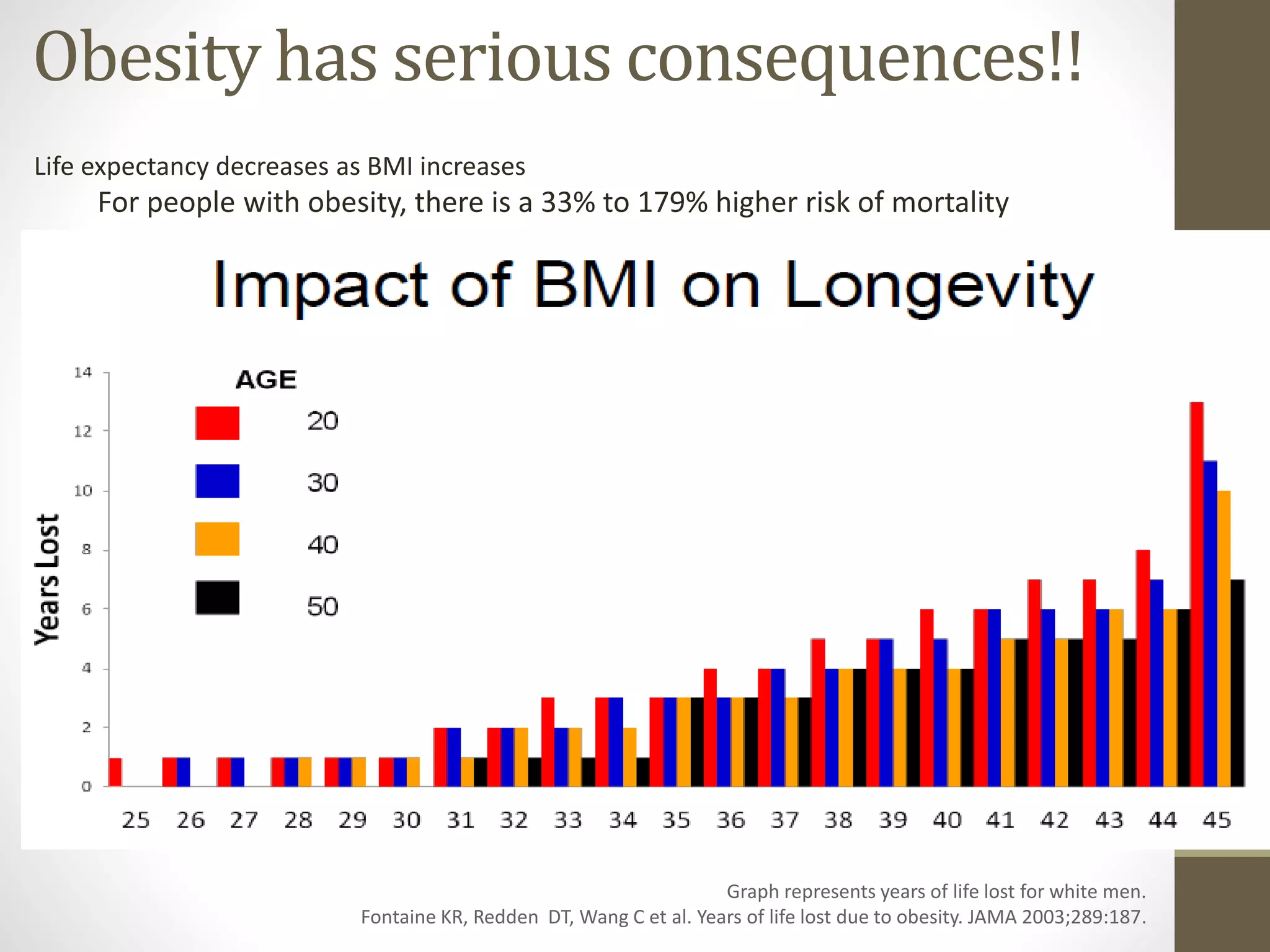
Obesity is a complex, multifactorial chronic disease linked to significant morbidity and mortality, affecting individual health outcomes and life expectancy. As body mass index (BMI) increases, so does the prevalence of serious health conditions such as diabetes, heart disease, and various cancers, with obesity-related healthcare costs exceeding $200 billion annually. The societal stigma against obesity also impacts psychosocial aspects of life, leading to decreased educational and employment opportunities, and a higher risk of depression.