Downloaded 1,540 times

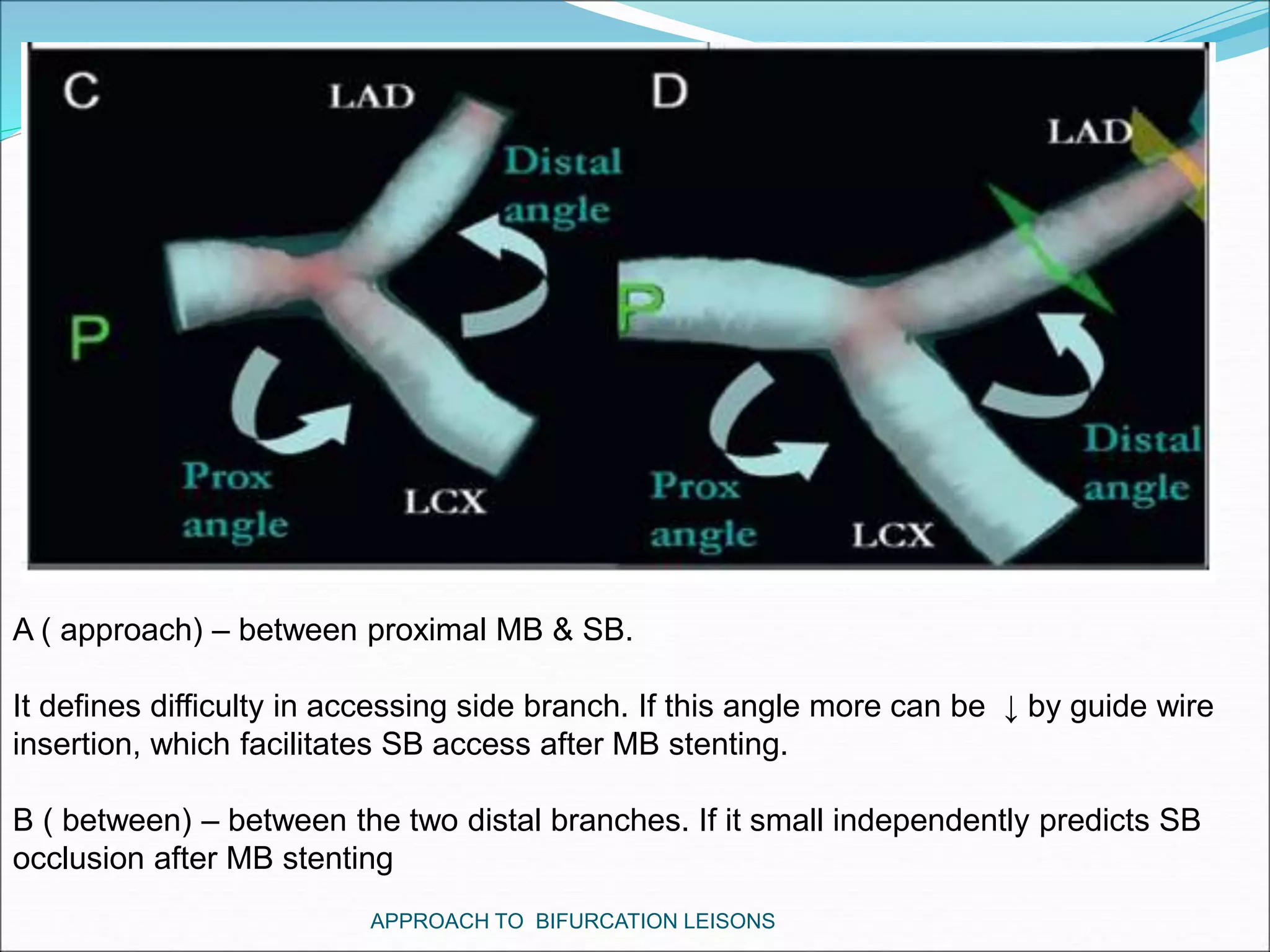








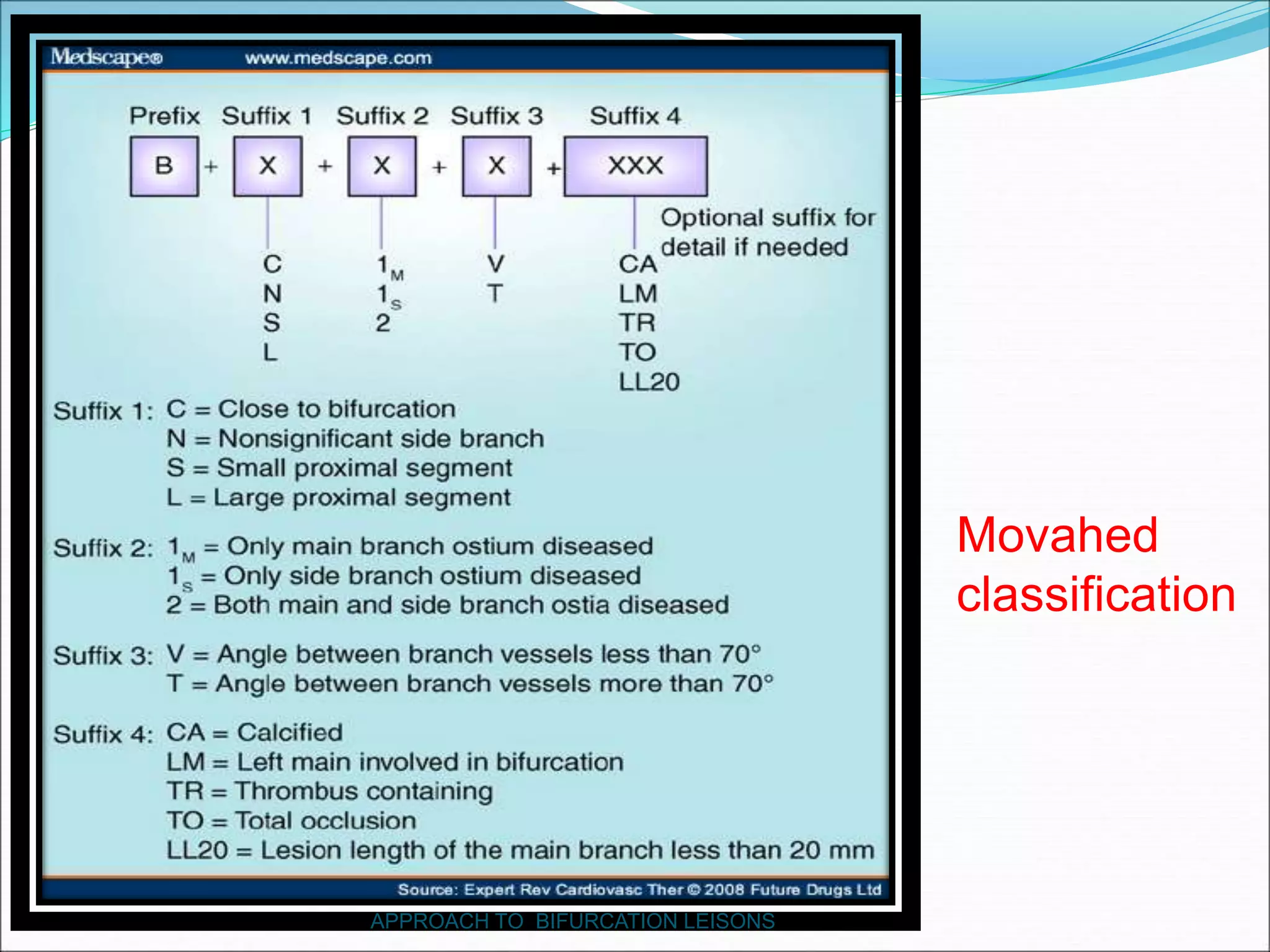

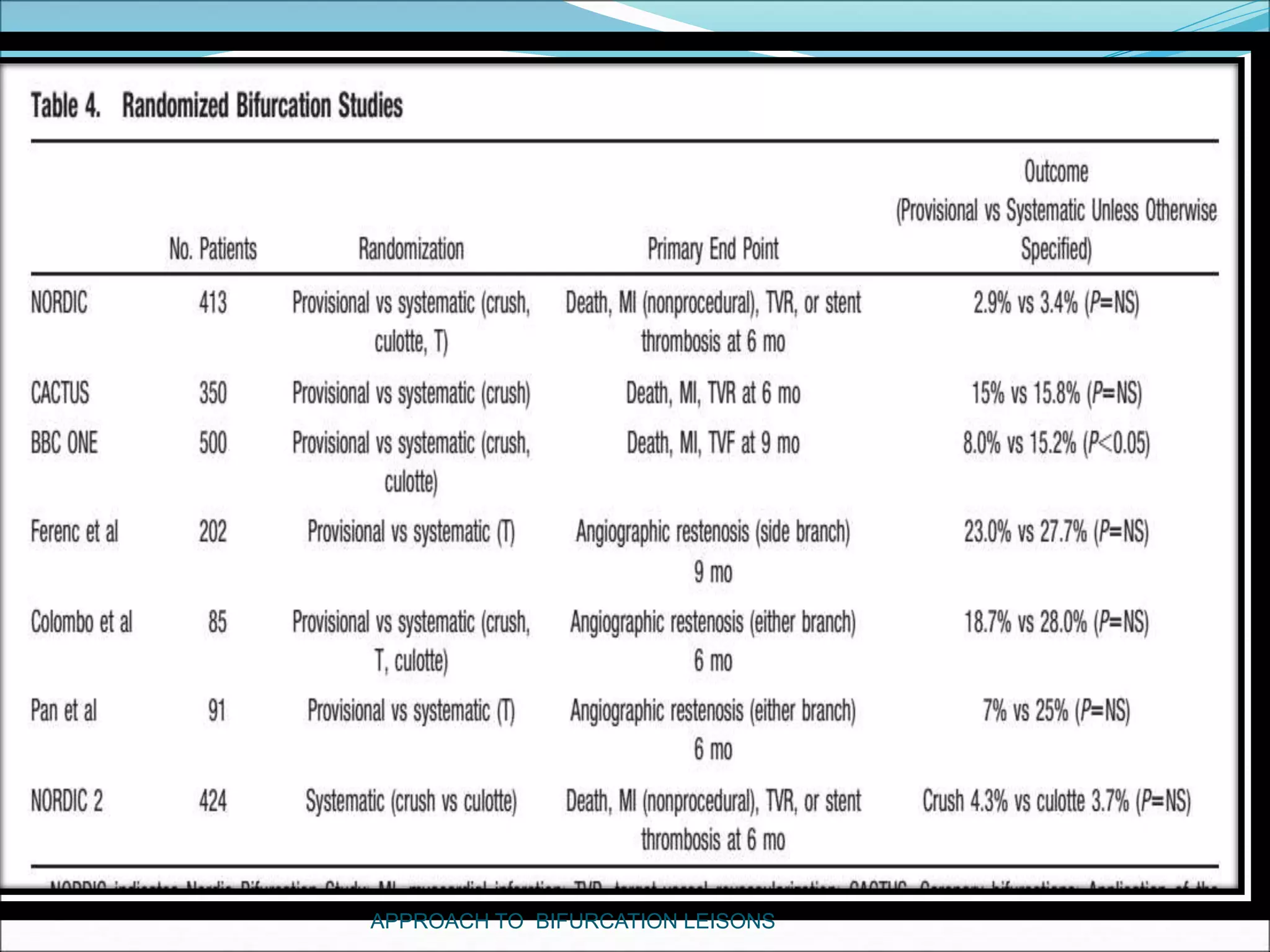
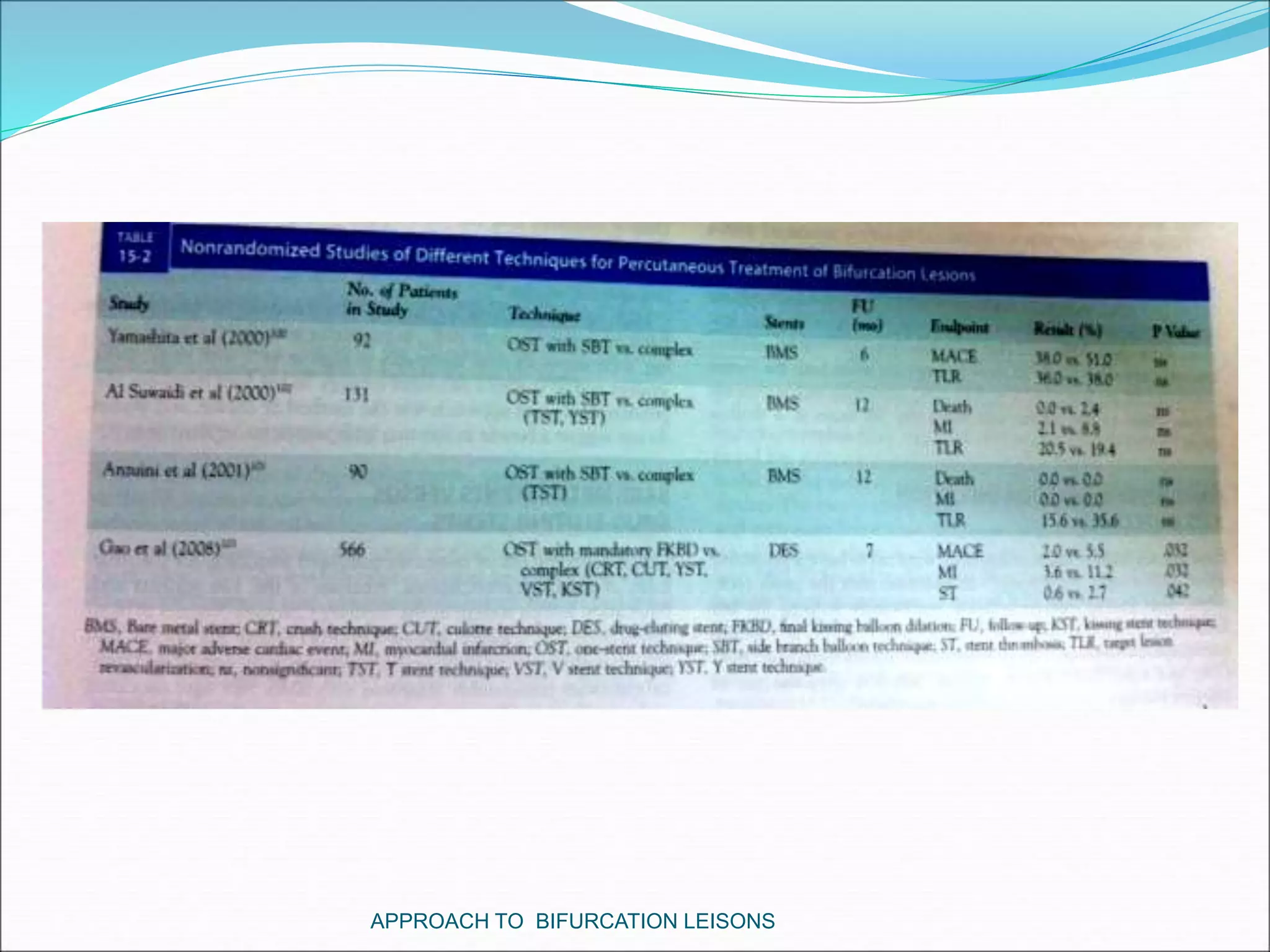
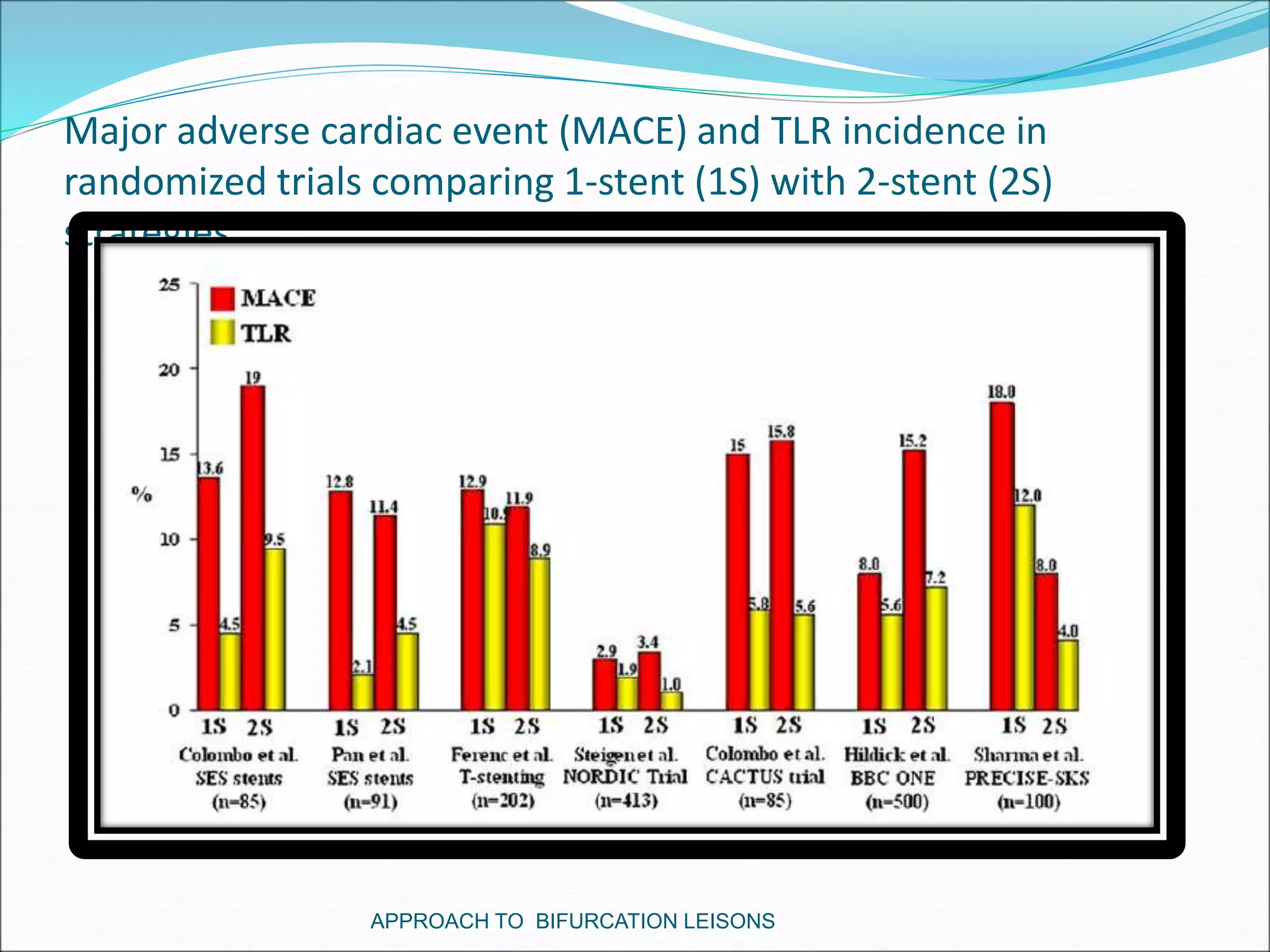





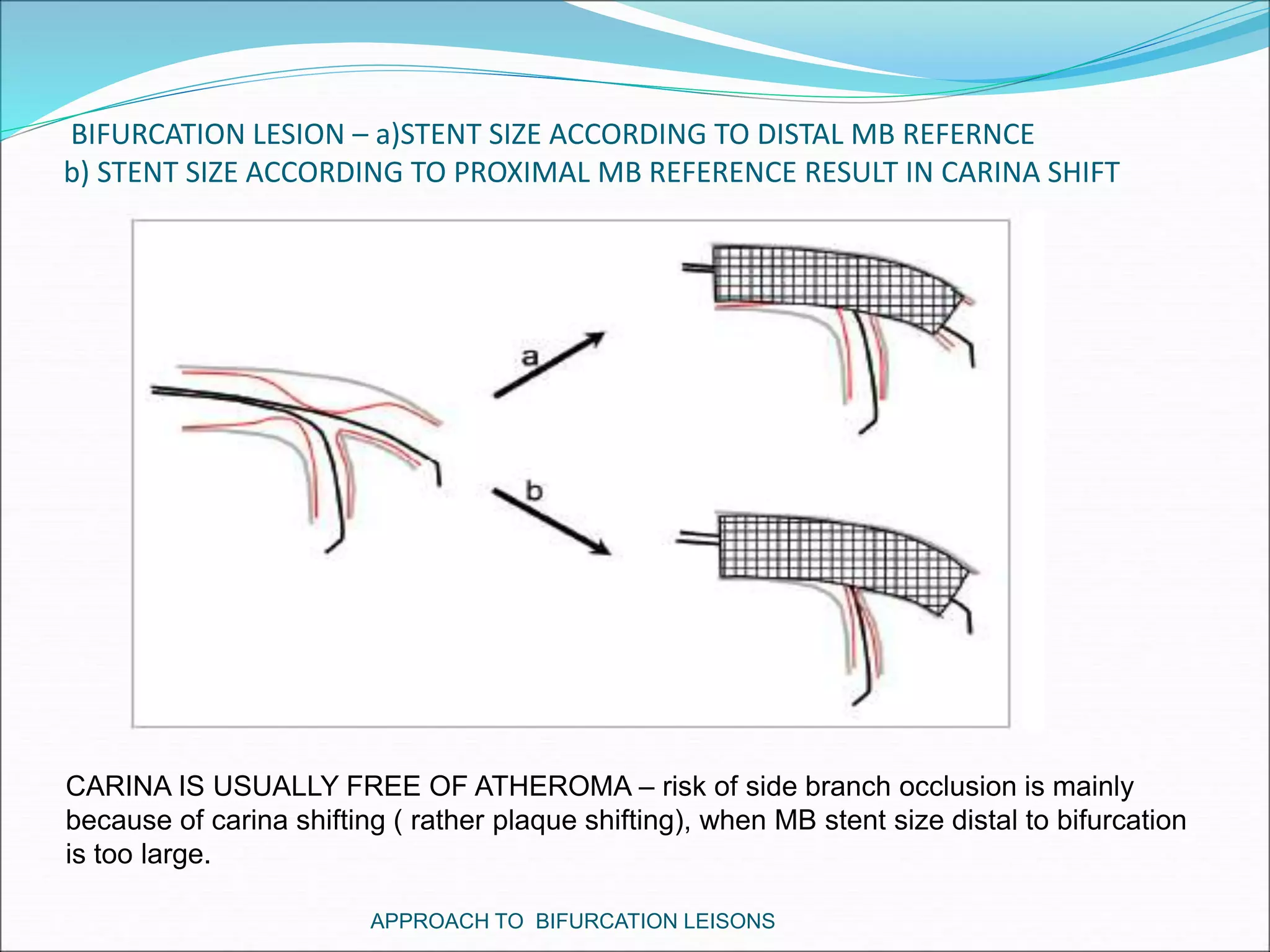
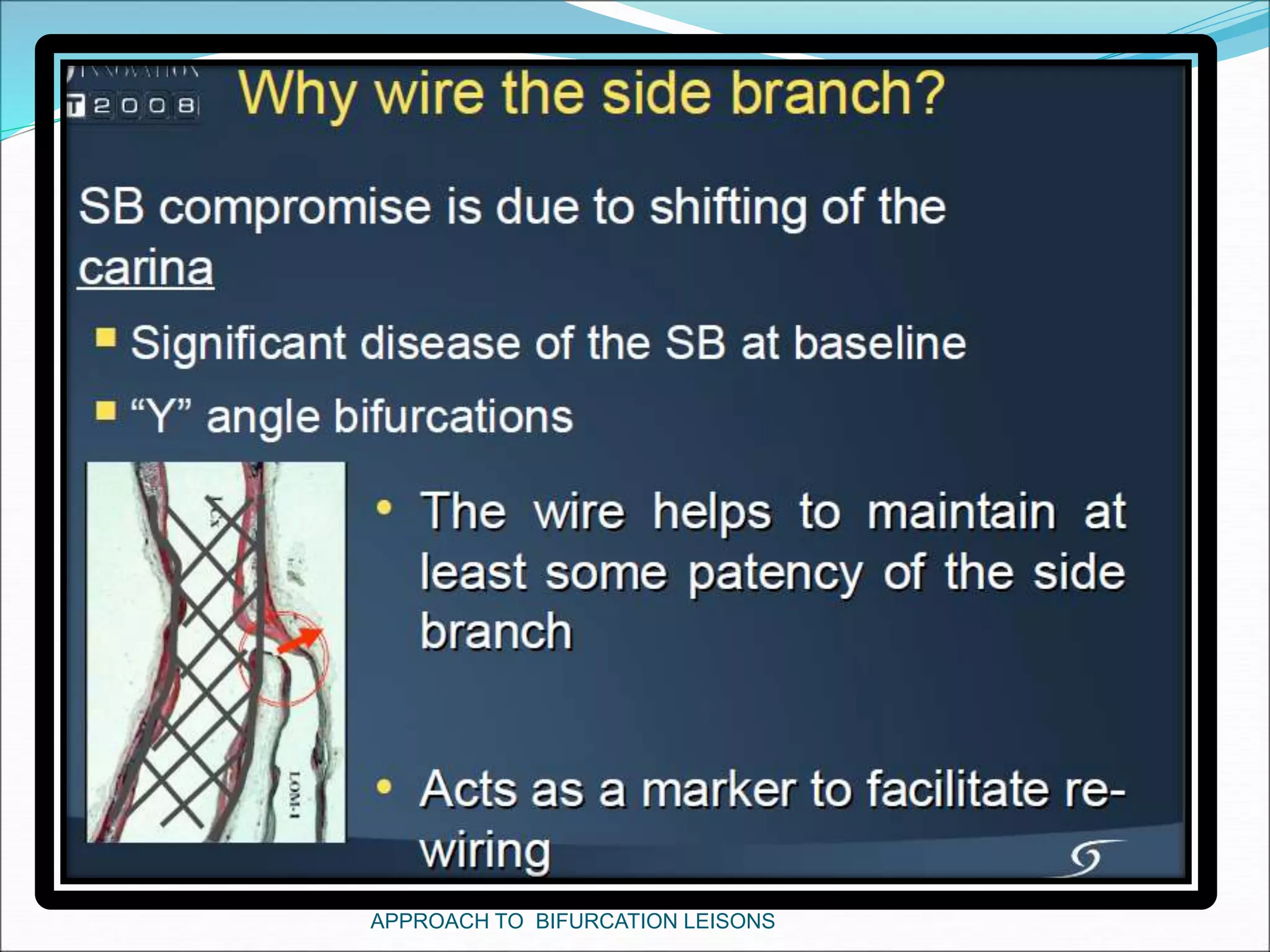
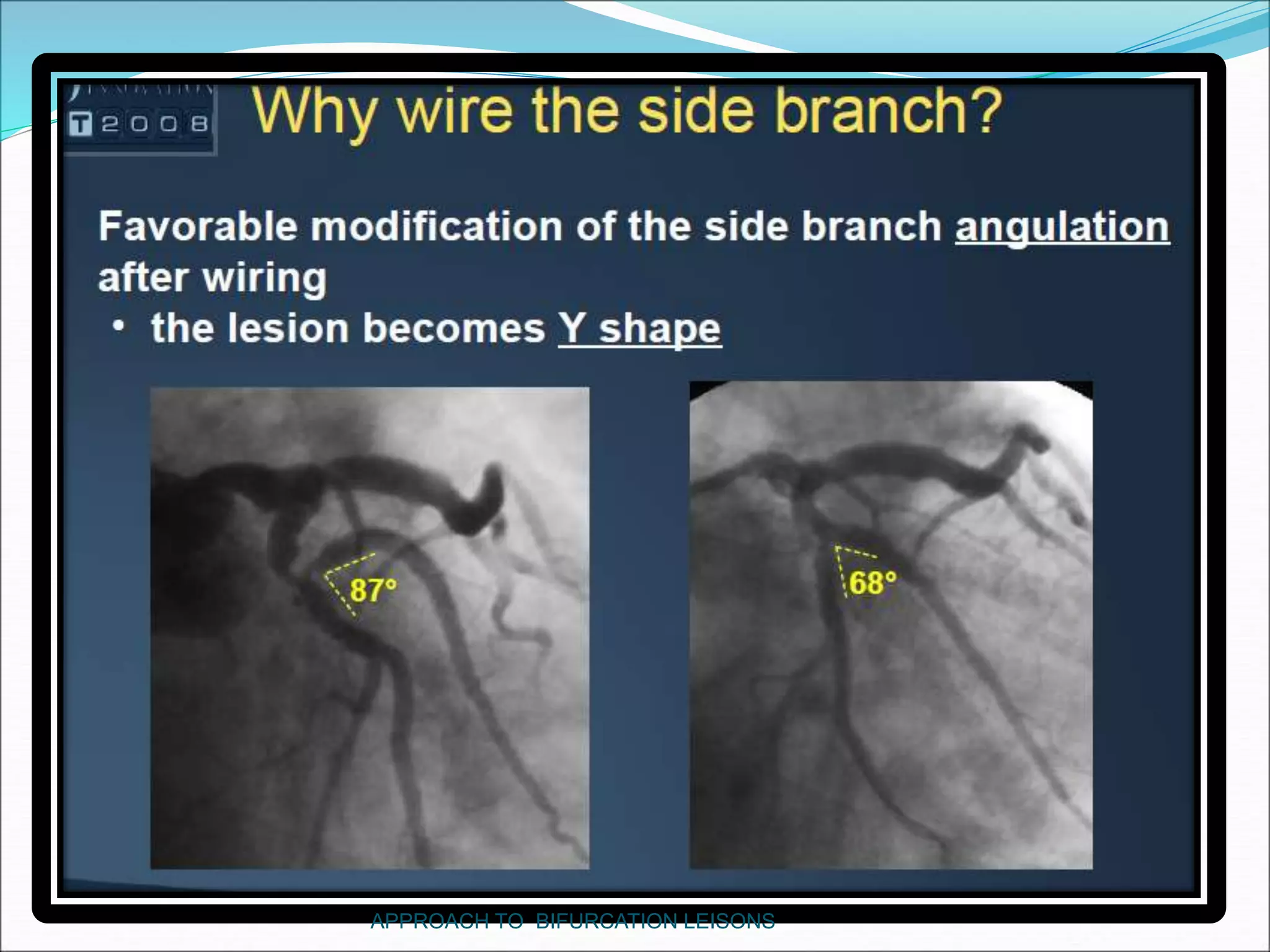













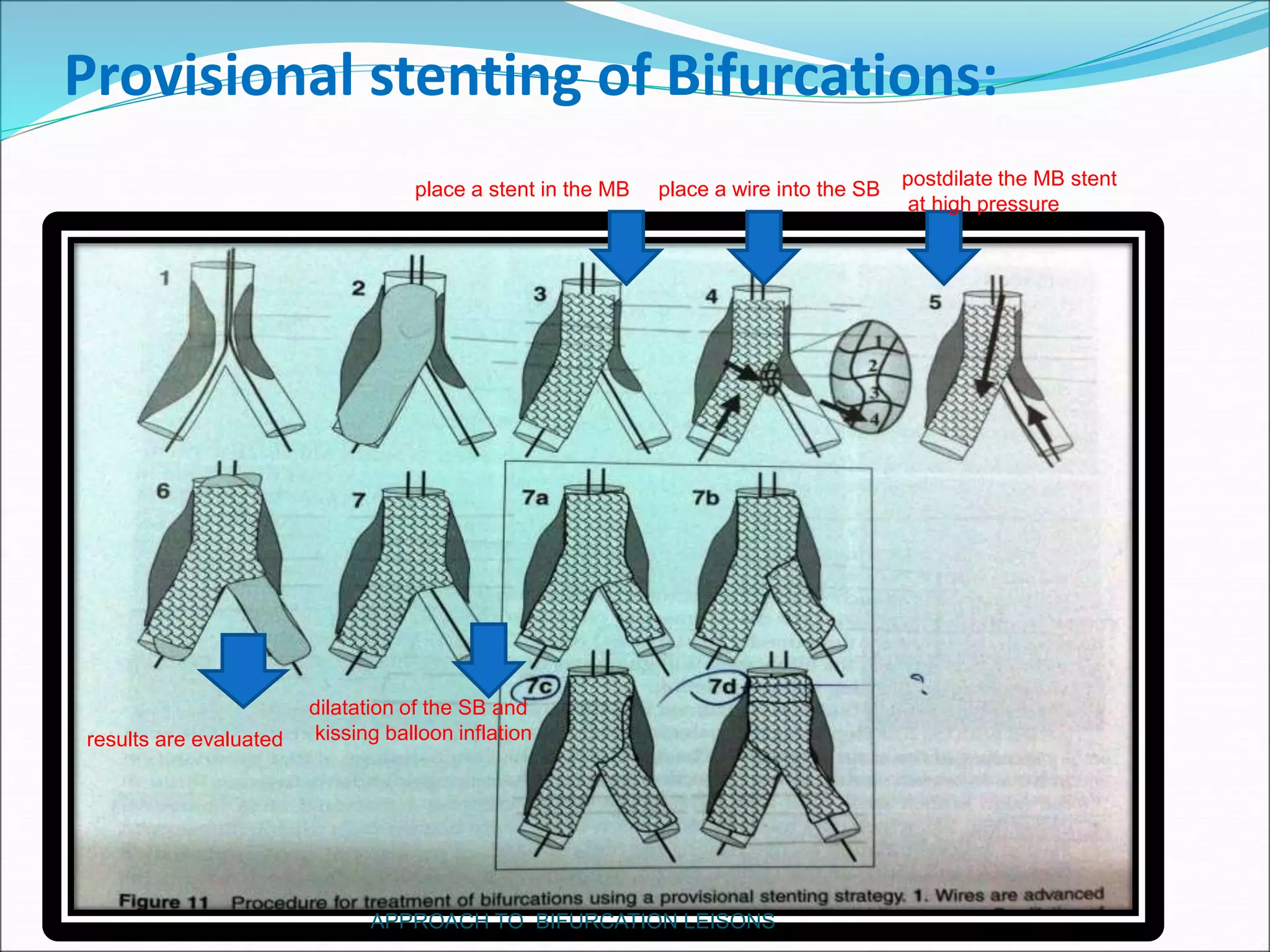
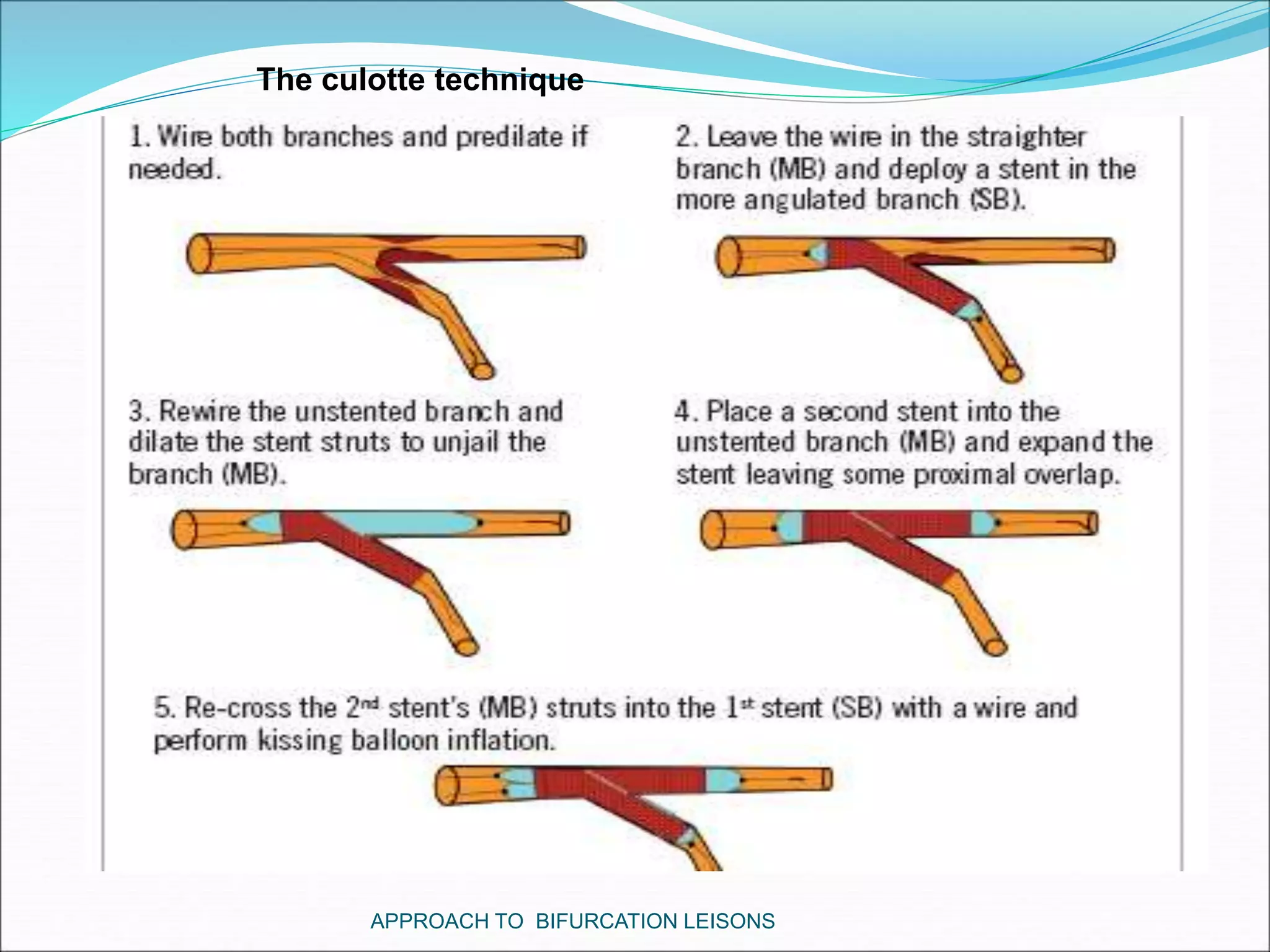


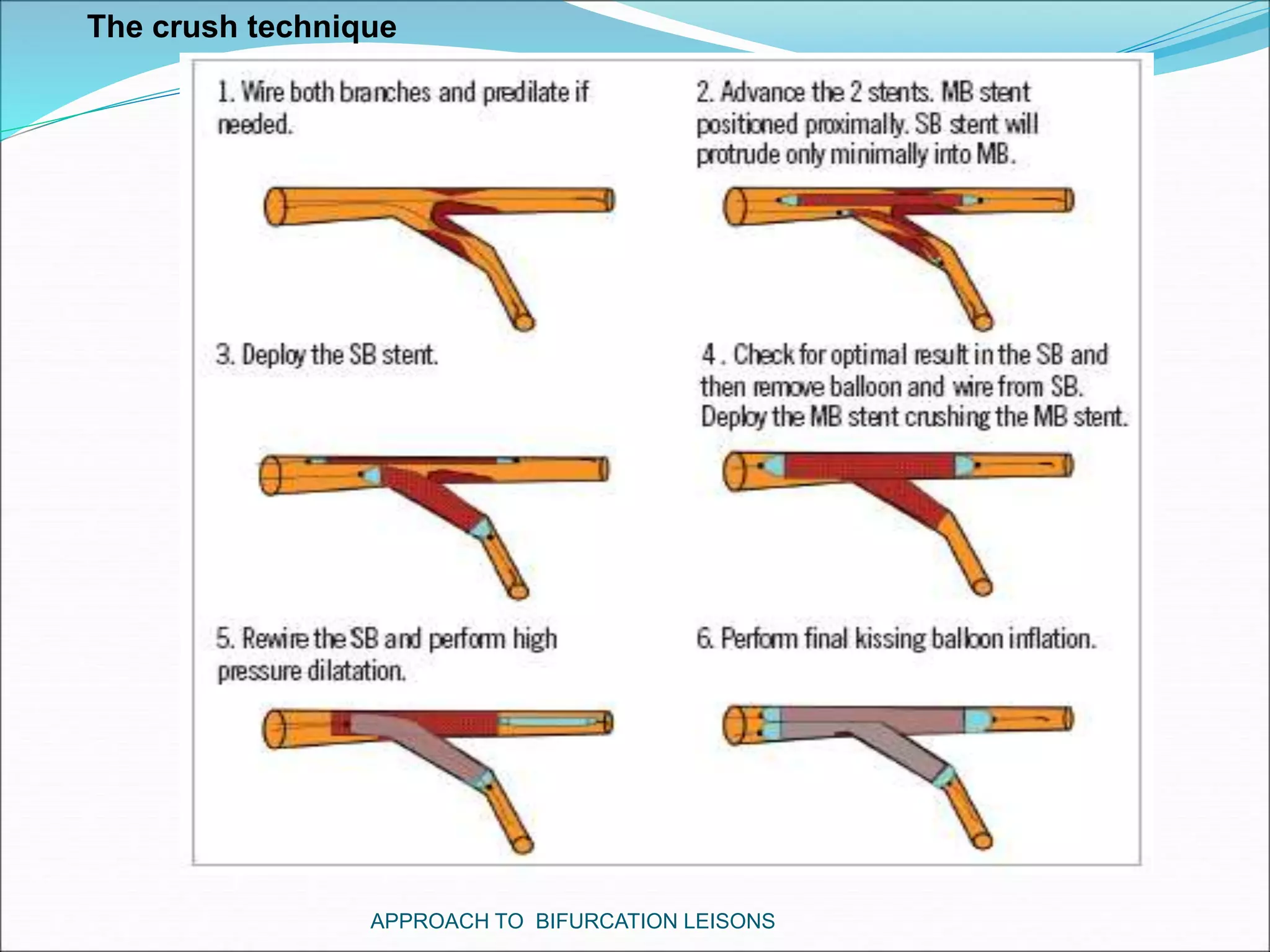


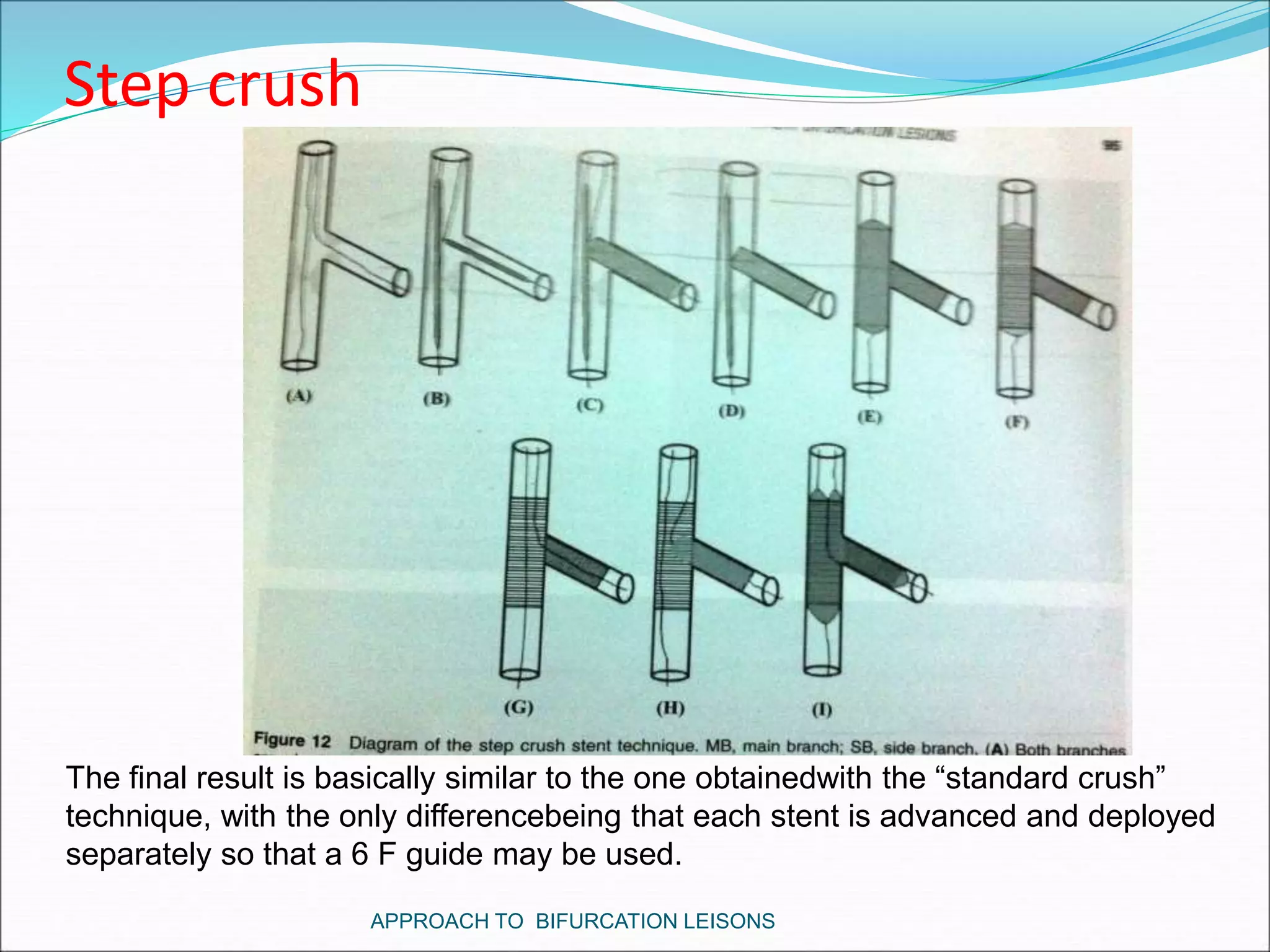






























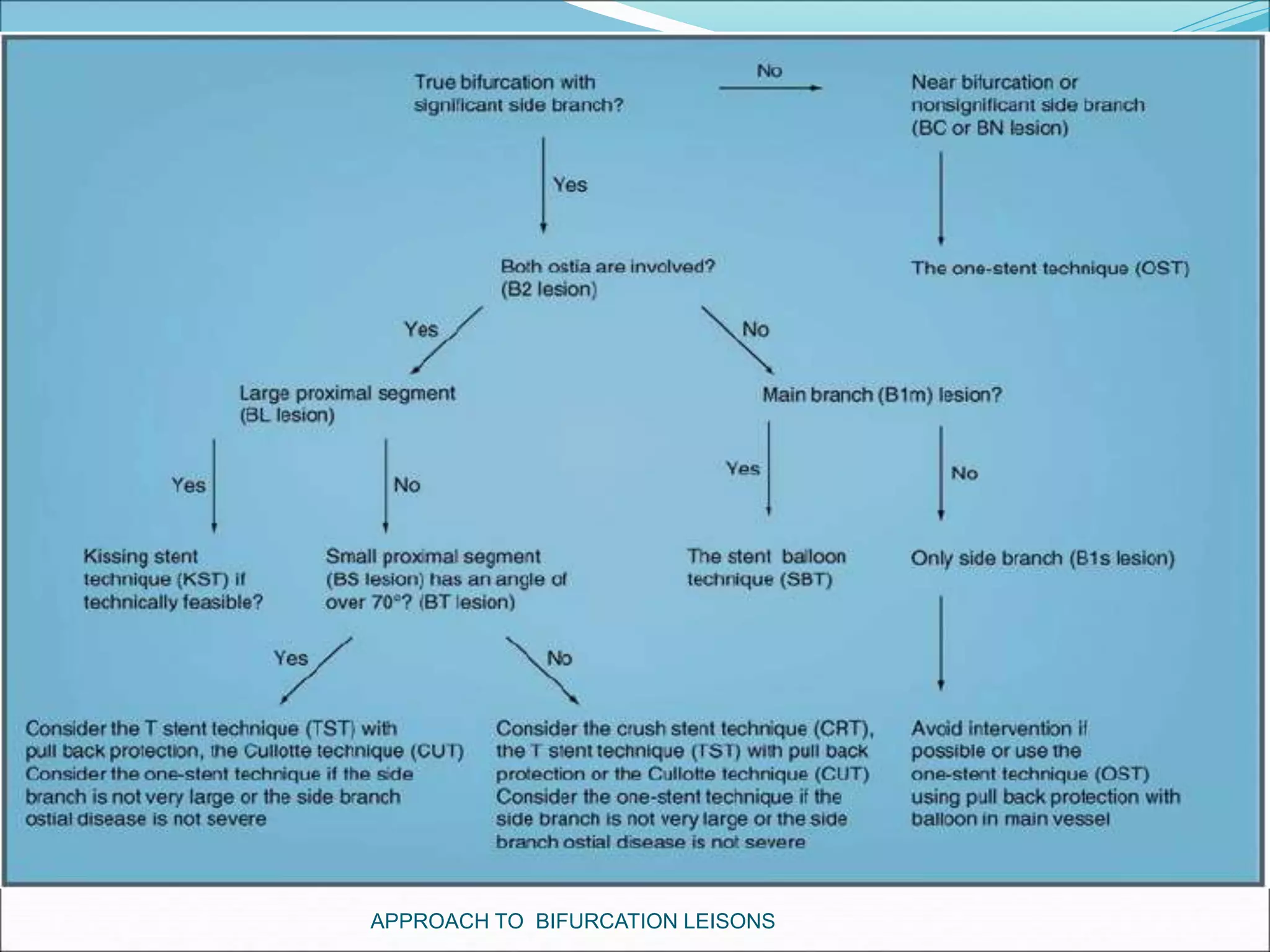

The document discusses approaches to bifurcation lesions in coronary arteries. It defines a bifurcation lesion as a lesion located at the bifurcation of a main branch and side branch. Some key points discussed include: - Provisional stenting of the main branch with adjunctive treatment of the side branch is generally the preferred initial approach. - Double stenting techniques like culotte stenting and crush stenting are more complex but may be needed for large side branches or complex lesions. - Factors like side branch size, angle of bifurcation, and extent of disease impact treatment decisions between single versus double stenting. - Techniques for wiring the side branch, optimizing stent placement, and treating























































































