

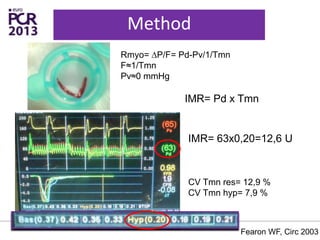
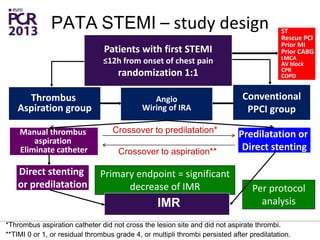
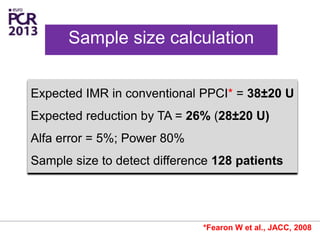
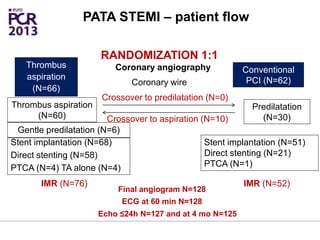
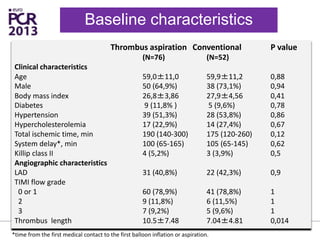

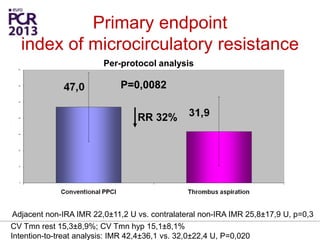
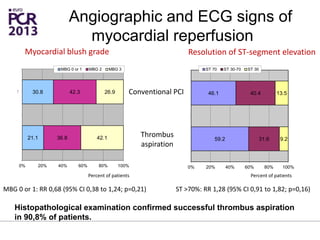
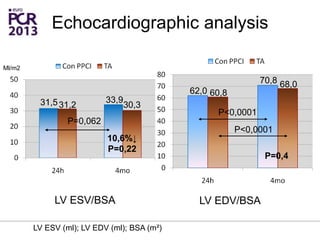
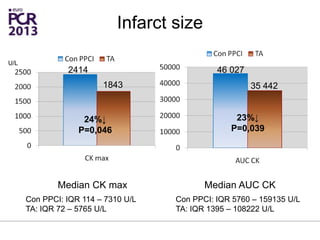
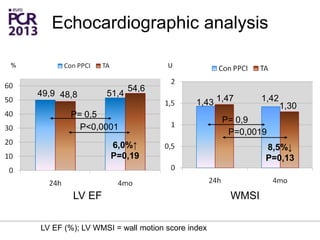
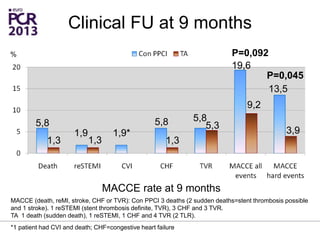
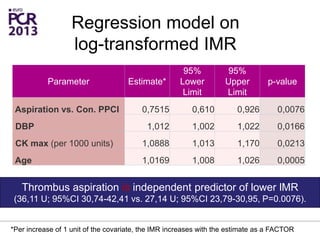
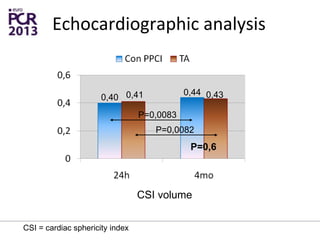
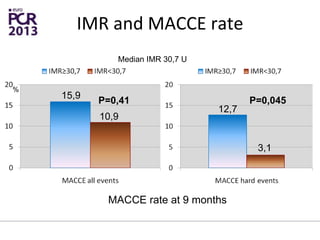
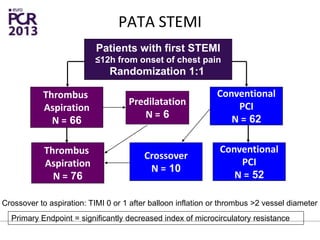
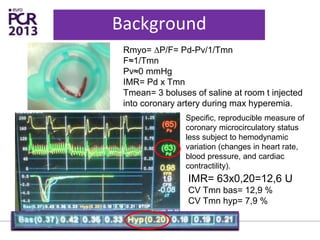
The PATA-STEMI study evaluates the impact of manual thrombus aspiration on myocardial perfusion in patients with first ST-segment elevation myocardial infarction (STEMI). Results indicate that thrombus aspiration significantly reduces the index of microcirculatory resistance compared to conventional percutaneous coronary intervention, reflecting improved myocardial perfusion. Additionally, at mid-term follow-up, adverse cardiac events were lower in the thrombus aspiration group, suggesting a potential clinical benefit, though further studies are recommended to confirm these findings.























































































