Downloaded 46 times
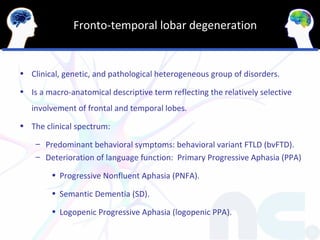
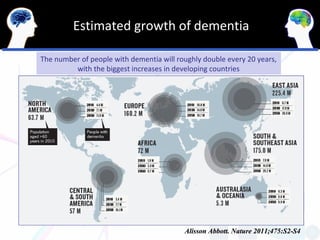
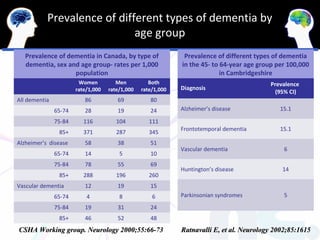
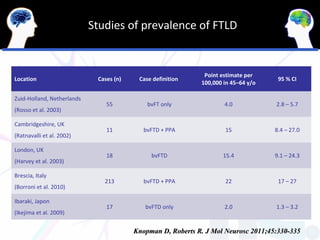
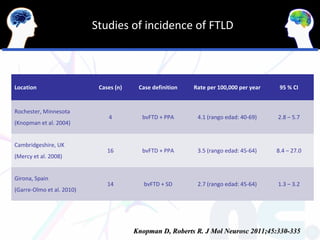
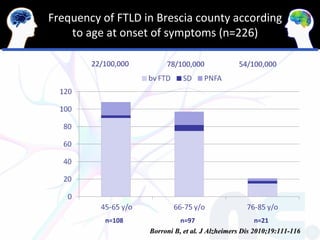
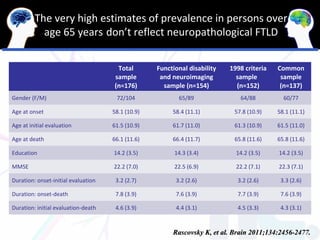
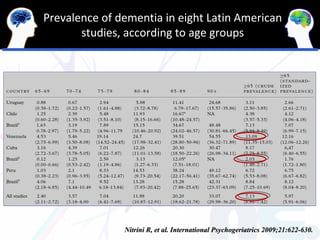
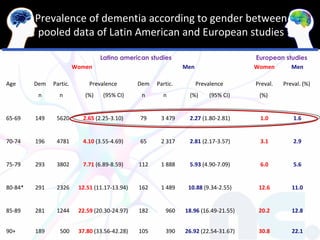
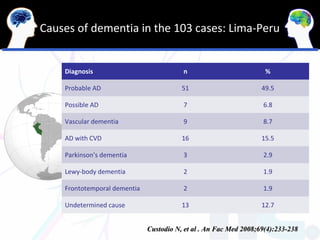
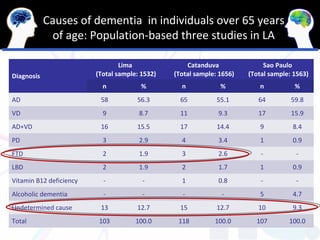
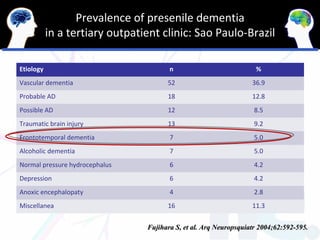
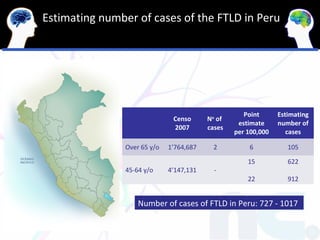
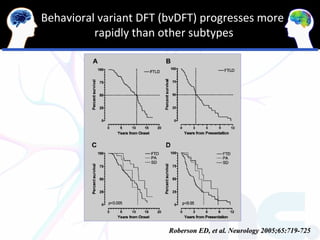
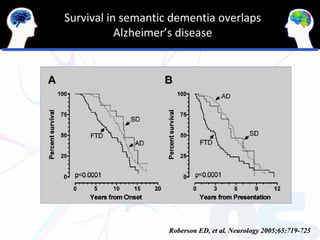
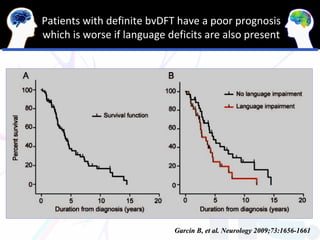


The document discusses clinical syndromes and epidemiology of frontotemporal lobar degeneration (FTLD) in Latin America. It outlines that the document will cover clinical syndromes of FTLD, prevalence and incidence of FTLD in LA, estimating number of FTLD cases in LA, mean survival time of FTLD, and economic impact of FTLD in LA. Studies in LA show the prevalence of dementia increases with age and is higher in women than men. Alzheimer's disease is the most common cause of dementia found in LA, followed by vascular dementia.



































































![Neurocognitive disorder [NCD]](https://cdn.slidesharecdn.com/ss_thumbnails/neurocognitivedisorderautosaved-201125072609-thumbnail.jpg?width=640&height=640&fit=bounds)



























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











