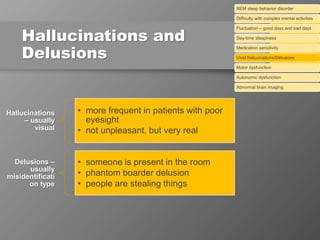
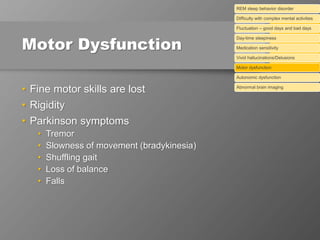
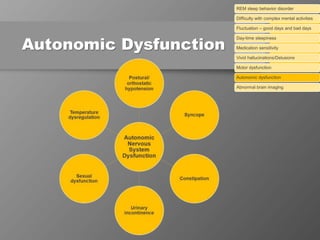
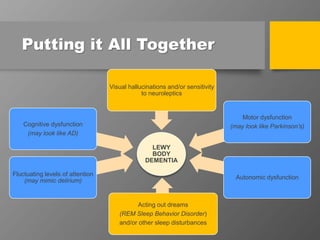
The document discusses dementia with Lewy bodies (DLB), highlighting its identification, symptoms, and management. It emphasizes the importance of recognizing DLB's unique features, including cognitive fluctuations and REM sleep behavior disorder, and the need for tailored treatment strategies to enhance quality of life for patients and alleviate caregiver burden. The document also addresses disparities in care and the significance of early diagnosis and comprehensive support.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















