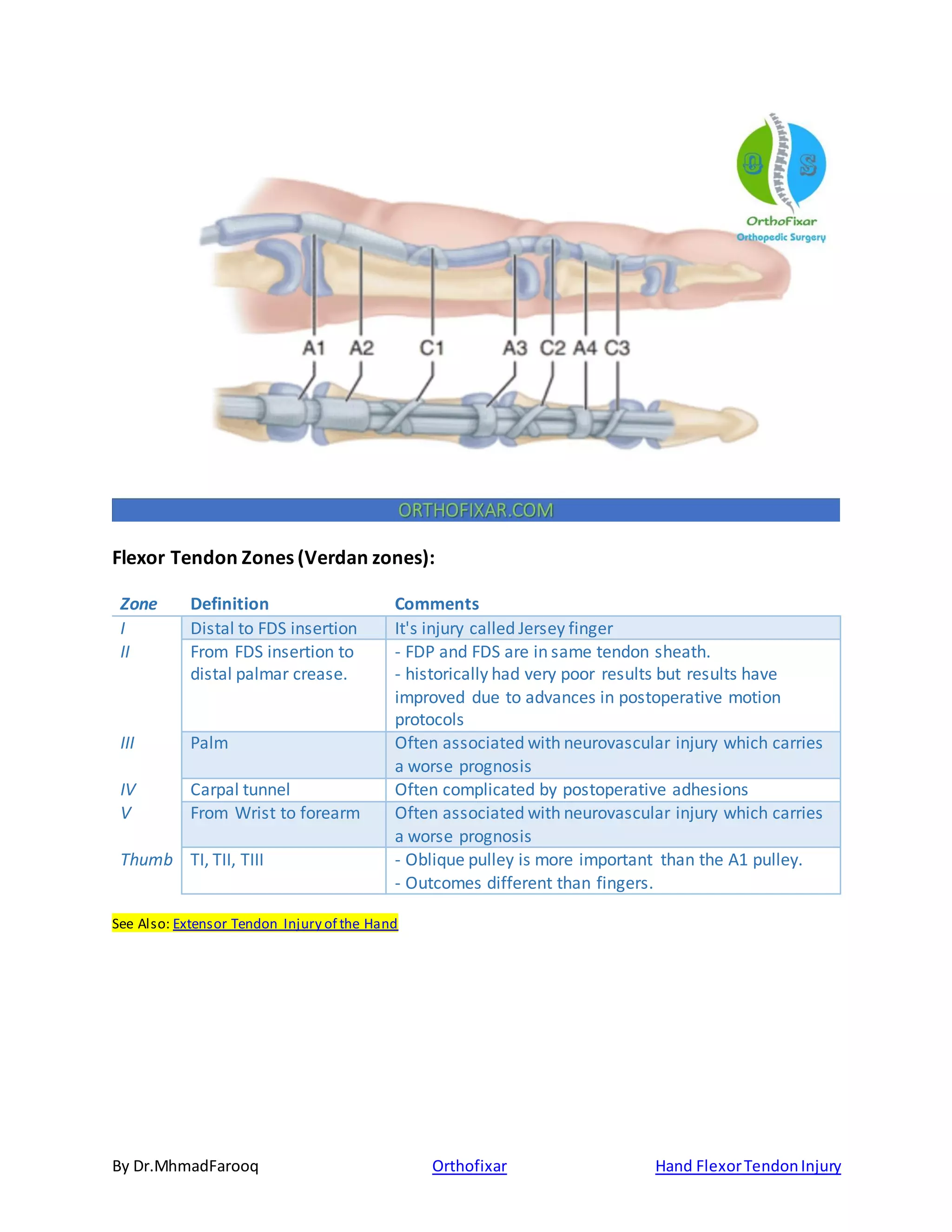
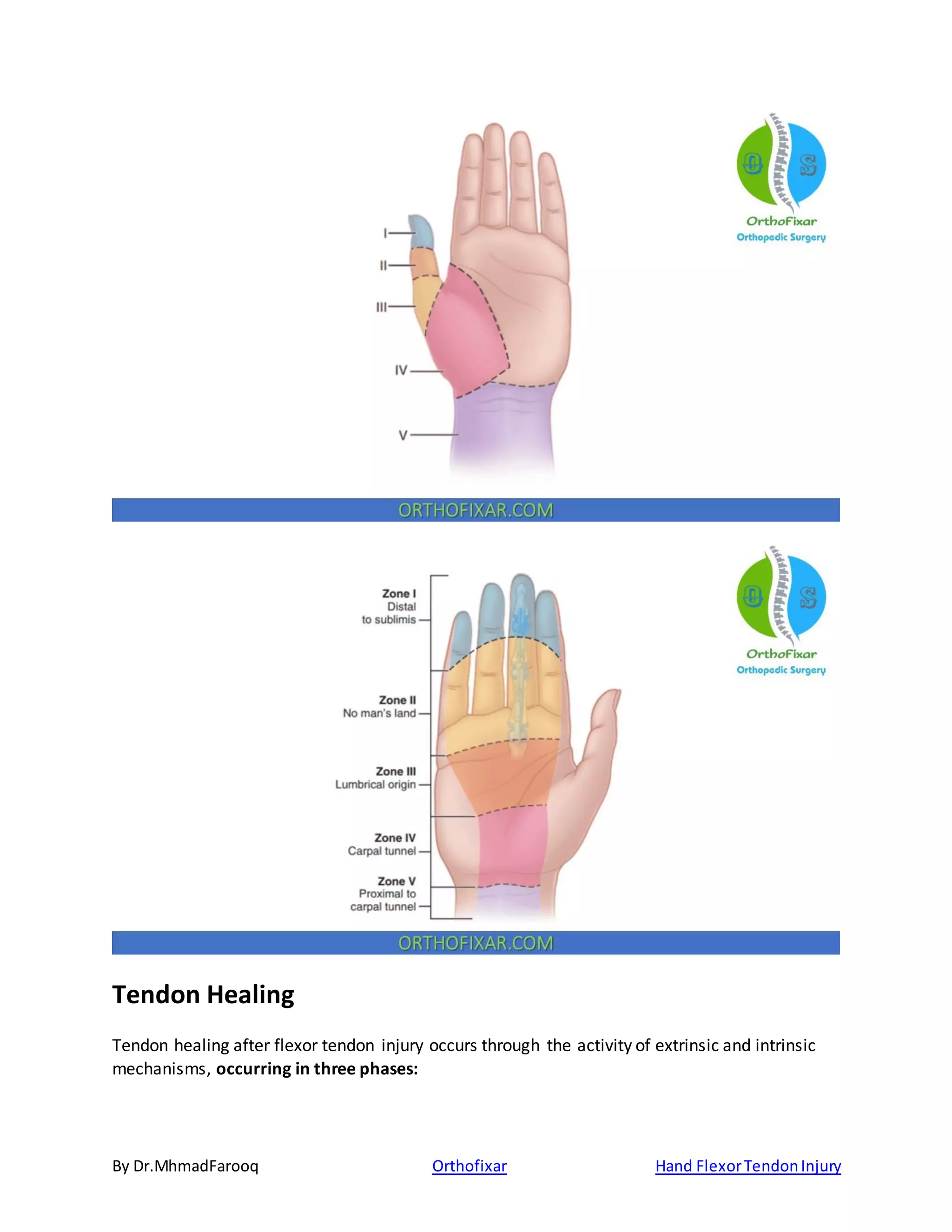
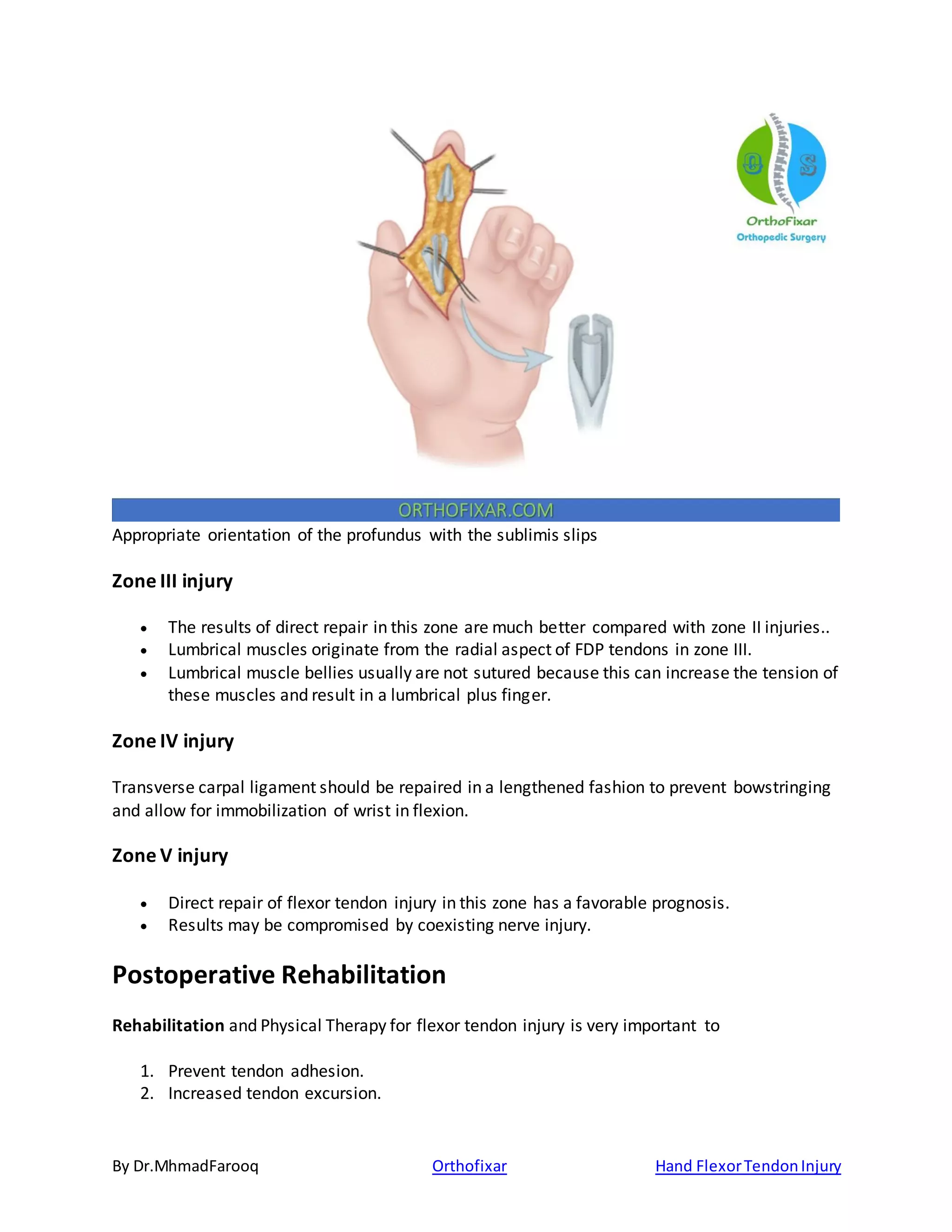
The document discusses hand flexor tendon injuries, which are common emergencies often caused by volar lacerations, detailing the anatomy, blood supply, zones of injury, healing process, clinical evaluation, and treatment options. It presents the need for careful classification of tendon injuries, emphasizing various repair techniques and rehabilitation protocols to optimize outcomes. Additionally, it highlights complications related to flexor tendon injuries, including adhesions, rerupture, and deformities.